
#12,102
Over the past 7 days 10 Chinese Provinces (plus Hong Kong ) have reported a total of 108 human H7N9 infections; Jiangsu (52 cases), Zhejiang (21 cases), Guangdong (14 cases), Anhui (9 cases), Jiangxi (5 cases), Shandong (2 cases), Fujian (1 case), Guizhou (1 case), Hunan (1 case) and Shanghai (1 case), and Hong Kong (1 case).
While we don't have the onset or diagnosis dates for these cases, the bulk are from December, and only yesterday announced. We haven't seen the NHFPC's monthly report, and so it is possible additional December cases could be announced.
Since we've been getting this information piecemeal, and with very little in the way of detail, we've been waiting for today's Hong Kong Avian Flu Report, hoping it will fill in some of the gaps. This is important because - most years - the H7N9 season doesn't really get started until January, and already we've exceeded last year's entire total.
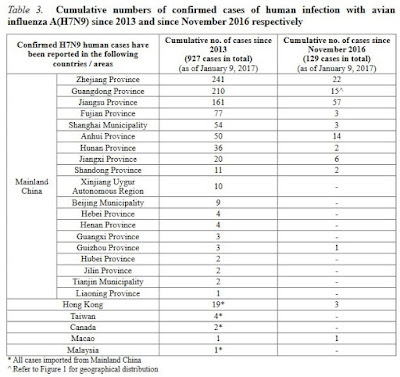
First a look at the Provincial Summary page, which has jumped from 21 cases reported on January 3rd, to 129 cases reported today, followed by their summary:
VOLUME 13, NUMBER 01
Reporting period: January 1, 2017 –January 7, 2017 (Week 01)
(Published on January 10, 2017)
Summary
1. Since the previous issue of Avian Influenza Report (AIR), there were 107 new human cases of avian influenza A(H7N9) reported by Mainland China health authorities in Jiangsu (52 cases), Zhejiang (21 cases), Guangdong (14 cases), Anhui (9 cases), Jiangxi (5 cases), Shandong (2 cases), Fujian (1 case), Guizhou (1 case), Hunan (1 case) and Shanghai (1 case). In addition, the Centre for Health Protection (CHP) of the Department of Health confirmed one human case of avian influenza A(H7N9). This case is the third case in Hong Kong this winter and the nineteenth case in Hong Kong. Since March 2013 (as of January 9, 2017), there were a total of 927 human cases of avian influenza A(H7N9) reported globally. Since November 2016 (as of January 9, 2017), 125 cases have been recorded in Mainland China. The latest case was reported on January 9, 2017.
2. Since the previous issue of AIR, there were no new human cases of avian influenza A(H5N6). Since 2014 (as of January 7, 2017), 16 human cases of avian influenza A(H5N6) were reported globally and all occurred in Mainland China. The latest case was reported on December 1, 2016.
3. There were no new human cases of avian influenza A(H5N1) reported by the World Health Organization (WHO) in 2017. From 2011 to 2015, 32 to 145 confirmed human cases of avian influenza A(H5N1) were reported to WHO annually (according to onset date). In 2016, there have been 10 cases in Egypt.*
* Since November 21, 2012, WHO only publishes information on human cases with avian influenza A(H5N1) infection in “Influenza at human - animal interface: Monthly Risk Assessment Summary”. Only cases of human infection with H5N1 involved in events that are unusual or associated with potential increased risks will be reported in Disease Outbreak News. The latest report was published in December, 2016.
Today's report also contains a case listing, with some basic demographic data on most of the cases, including age, gender, province, and condition. There are a few gaps in this data, with some cases listed as `Under Investigation'.
As we go through this data, it is important to remember the general demographics of China. Half the population (675+ million) are under the age of 37, while females make up a little more than 48% of the population (see chart below).
 |
| Credit Wikipedia |
But you'd never know it from the demographics of today's report.
- Of the 107 cases where we know the gender, 69 are male (63%) and 38 are female (37%).
- Among one of the largest decade demographic age group (20-29) in China, only one case (age 23) is reported). No other cases younger than 30 were reported at all.
- Only 7 of the 108 cases (6.4%) reported fell at or below the median age (37) in China.
Another thing that jumps out from this report is just how many are listed as either fatal, critical, or suffering from `Severe Pnuemonia'. Out of 108 cases (including Hong Kong):
- 2 are listed in `Stable' condition
- 34 have died
- 47 are listed with `Severe Pneumonia'
- 8 are listed with `Pneumonia'
- 5 are listed as `Critical'
- and the rest are either unstated or still under investigation
Regardless, what we aren't seeing are any cases described as `mildly' ill, and very few that are considered `stable'.
That said, only the `sickest' of the sick tend to turn up at hospitals and end up tested, so there are likely a number of mild or moderately ill cases in the community that are not picked up by surveillance.
This dramatic age shift to patients predominantly over 40, and high fatality rate and large number of patients described as having `Severe Pneumonia', suggests that the virus may be exacting a much greater toll on patients with comorbidities, or lowered immunity, both of which tend to increase with age.
Only one case under the age of 30, however, is pretty remarkable.
While age, and comorbidities may be the determining factors, last November in Science: Protection Against Novel Flu Subtypes Via Childhood HA Imprinting, we looked at another intriguing theory; that the first influenza subtype you are exposed to makes the biggest, and most lasting, impression on your immune system.
And that the resultant immune response may carry over to other - similar - subtypes.
Simply put, if your first influenza exposure was to H1N1 or H2N2 (group 1 influenza viruses), you may carry some degree of immunity to the H5 viruses (H5N1, H5N6, etc.). If, however, your first exposure was to H3N2 (group 2), you may carry some protection against H7N9 instead.
Those born before 1968 would have been first exposed to group 1 influenza viruses, and would theoretically have more immunity against H5 subtypes, while those born between 1968 and 1977 would have been mostly likely have been first exposed to an H3 (group 2) virus.
Those born after 1977 could have been exposed first to either one.
Lending some credence to this theory, the history with H5N1 has been it has infected far more children and adolescents than adults, while H7N9 has affected mostly older adults. Although an attractive and elegant explanation, there's a lot more work needed to validate it.
Of course, there is rarely just one factor that determines how a virus affects a given population. Gender differences may be due to exposure risks, age shifts may be due to HA imprinting, comorbidities, lowered immune systems, or some other reasons we don't yet fathom.
Any way you slice it, we've a lot more to learn about the H7N9 virus, and the threat it poses to public health.