
#12,707
Fourteen months ago (June 24th, 2016) the CDC issued a Clinical Alert to U.S. Health care facilities about the Global Emergence of Invasive Infections Caused by the Multidrug-Resistant Yeast Candida auris.
C. auris is an emerging fungal pathogen that was first isolated in Japan in 2009. It was initially found in the discharge from a patient's external ear (hence the name `auris'). Retrospective analysis has traced this fungal infection back over 20 years.
Since then the CDC and public health entities have been monitoring an increasing number of cases (and hospital clusters) in the United States and abroad, generally involving bloodstream infections, wound infections or otitis (see July Update).
Last week the CDC promoted the first ever Fungal Disease Awareness Week, and last Tuesday presented a COCA call webinar called Tackling an Invasive, Emerging, Multi-drug Resistant Yeast: Candida auris — What Healthcare Providers Need to Know, which is now archived and available online.
Overview
Candida auris, an emerging multidrug resistant fungus that can cause invasive infections with high mortality, has been associated with outbreaks in healthcare settings. C. auris was first described in 2009, after being isolated from external ear canal discharge of a patient in Japan. Since then, reports of C. auris infections, including bloodstream infections, have been noted from over a dozen countries—and it has now been found in the United States. As of July 14, 2017, 98 cases have been reported to CDC.
The emergence of C. auris raises several serious concerns for public health. First, many isolates are multidrug-resistant, with some strains having elevated minimum inhibitory concentrations to drugs in all three major classes of antifungal medications, a feature not found in other clinically relevant Candida species. Second, C. auris is challenging to identify, requiring specialized methods like MALDI-TOF or ribosomal DNA sequencing. When using common biochemical methods such as analytical profile index strips or the VITEK 2, C. auris is often misidentified as other yeasts (most commonly Candida haemulonii, but also Candida famata, Rhodotorula glutinis). Finally, C. auris has caused outbreaks in health care settings, spreading from patient to patient, and contaminating healthcare environments. During this COCA call, clinicians will learn about the updated identification, treatment, and infection control recommendtions for C. auris.
Slides: View Now Audio: Listen Now Webcast: Watch Now
The following day CIDRAP's Antimicrobial Stewardship Project (ASP) held an hour long webinar (see below), which is now available on the CIDRAPASP Youtube channel.
 |
| https://www.youtube.com/watch?v=gCO7kWdnbkY |
(Note: you'll find more than a dozen other on-topic videos available on this channel as well).
Yesterday the CDC updated their C. Auris surveillance page, where they now show 112 cases reported across 8 states, and the number of colonized asymptomatic cases has risen to 120.
August 21, 2017: Case Count Updated as of July 31, 2017
What's New?
Candida auris is an emerging fungus that presents a serious global health threat. Healthcare facilities in several countries have reported that C. auris has caused severe illness in hospitalized patients. Some strains of C. auris are resistant to all three major classes of antifungal drugs. This type of multidrug resistance has not been seen before in other species of Candida. Also of concern, C. auris can persist on surfaces in healthcare environments and spread between patients in healthcare facilities. CDC has developed identification, treatment, and infection control recommendations to help prevent the spread of C. auris.
- August 21, 2017: case count updated to 112
- July 14, 2017: Updated recommendations on identification, treatment, and infection control
- June 26, 2017: Fact Sheet on Candida auris
- May 18, 2017: MMWR Notes from the Field on ongoing transmission
CDC encourages all U.S. laboratory staff who identify C. auris to notify their state or local public health authorities and CDC at candidaauris@cdc.gov.
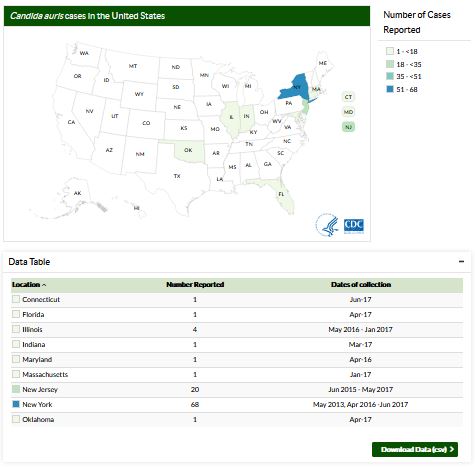
Location represents the state of C. auris specimen collection. The case counts displayed reflect clinical cases of C. auris (i.e., based on specimens collected in the normal course of care). They do not include patients who screened for presence of C. auris colonization. C. auris has been isolated from an additional 120 patients from healthcare facilities in 4 states where clinical cases were detected. This map will be updated monthly.Resources
(Continue . . . )
- General Information about Candida auris
- Recommendations for Identification, Treatment, and Infection control of Candida auris
- June 2016 Clinical Alert: Information for Healthcare Professionals about Candida auris
- Laboratory Submission Information
Some earlier blogs on this emerging pathogen include:
MMWR: Ongoing Transmission of Candida auris in Health Care Facilities
MMWR: Investigation of the First Seven Reported Cases of Candida auris In the United States
mSphere: Comparative Pathogenicity of UK Isolates of the Emerging Candida auris