 |
| Credit CDC |
#13,162
Lassa fever is a Viral Hemorrhagic Fever (VHF) endemic to a handful of West African nations - commonly carried by multimammate rats - a local rodent that often likes to enter human dwellings.
Exposure is typically through the urine or dried feces of infected rodents, and roughly 80% who are infected only experience mild symptoms.The incubation period runs from 10 days to 3 weeks, and the overall mortality rate is believed to be in the 1%-2% range, although it runs much higher (15%-20%) among those sick enough to be hospitalized.
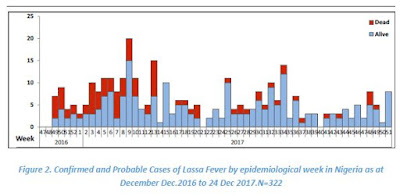
Although endemic in West Africa, between 2013 and early 2016 Nigeria had seen a steady decline in the number of Lassa Fever cases - and deaths - with the last significant outbreak reported in 2012.
But in early 2016 that trend began to change with outbreaks starting in Nigeria (see Nigeria: Lassa Fever Outbreak With 40 Fatalities), and then flaring up in both Benin and Togo (see ECDC: Rapid Risk Assessment On Lassa Fever In Nigeria, Benin, Togo, Germany & USA).Exported cases turned up in Germany and Sweden (see Germany's RKI Statement On Lassa Fever Cluster In Cologne & WHO Lassa Fever Update - Sweden (Imported)). Although Lassa reports in Nigeria eventually slowed, by December of 2016 they were on the rise again, and were fairly consistent through 2017 (see chart below).
Beginning in early January of 2018 those numbers began to increase markedly again (see chart below).

Some excerpts from the latest (week 7) Epidemiological report from the Nigerian CDC:

HIGHLIGHTS
- In the reporting Week 07 (February 12-18,2018) sixty eight new confirmediI cases were recorded from seven States Edo (35), Ondo (19), Bauchi (1), Ebonyi (7), Anambra (4), Imo(1) and FCT (1) with four new deaths in confirmed cases from two states Ondo (2), and Bauchi (2)
- From 1st January to 18th February 2018, a total of 913 suspected cases, and 73 deaths have been reported from 17 activeiv States- (Edo, Ondo, Bauchi, Nasarawa, Ebonyi, Anambra, Benue, Kogi, Imo, Plateau, Lagos, Taraba, Delta, Osun, Rivers, FCT, and Gombe) - Figure 1
- Since the onset of the 2018, 277 cases have been classified as: 272 confirmed cases, 5 probable cases with 59 deaths (54 in Lab confirmed and 5 in probable) -Table 1
- Case Fatality Rate in confirmed and probable cases is 21%
- Fourteen Health Care workers have been affected in six states –Ebonyi (7), Nasarawa (1), Kogi (1), Benue (1), Ondo (1) and Edo (3) with four deaths in Ebonyi (3) and Kogi (1)
- Predominant age group affected is age group 30-50 (Median Age = 32) - Figure 4
- The male to female ratio for confirmed cases is 2:1
- 74% of all confirmed cases are from Edo (45%) and Ondo (29%) states
- National RRT team (NCDC staff and NFELTP residents) batch A replaced with batch B to continue response support in Ebonyi, Ondo and Edo States
- Irrua Specialist Hospital has 39 cases on admission this weekend. FMC Owo has 29 isolation beds, all occupied.
- A total of 2351 contacts have been identified from 17 active states and 1747 are currently being followed up
- Joint NCDC and WHO team on high level visit to Edo, Ondo and Ebonyi states
- NCDC is collaborating with ALIMA and MSF in Edo, Ondo and Anambra States to support case management
- NCDC deployed teams to four Benin Republic border states (Kebbi, Kwara, Niger and Oyo) for enhanced surveillance activities
- National Lassa fever multi-partner multi-agency Emergency Operations Centre(EOC) continues to coordinate the response activities at all levels
(Continue . . . )
Like many other hemorrhagic fevers, person-to-person transmission may occur with exposure to the blood, tissue, secretions, or excretions of an individual, although the CDC reassures:
Casual contact (including skin-to-skin contact without exchange of body fluids) does not spread Lassa virus. Person-to-person transmission is common in health care settings (called nosocomial transmission) where proper personal protective equipment (PPE) is not available or not used. Lassa virus may be spread in contaminated medical equipment, such as reused needles.While likely to remain primarily a localized public health threat, we've seen exported cases before, and in 2016 the ECDC offered the following advice to travelers to the region.
Advice to travellers
Travellers to West Africa should be informed of the risk of exposure to Lassa fever virus, particularly in areas currently experiencing outbreaks. The risk is higher in rural areas where living conditions are basic.
Travellers should avoid consumption of foods and drink contaminated by rodent droppings, exposure to rodents or to patients presenting with haemorrhagic fever.
People travelling to these regions to provide care should be aware of the risk of exposure and should apply appropriate personal protective measures.