
# 8680
The journal Eurosurveillance has published a detailed rapid communications on the two related - imported (from KSA) - cases of MERS to the Netherlands reported earlier this month (see here & here).
There is far too much information here to excerpt efficiently, so I’ll simply post the abstract, the link, and a snippet from the discussion – but I would invite you to read it in its entirety on the Eurosurveillance site.
Eurosurveillance, Volume 19, Issue 21, 29 May 2014
Rapid communications
M Kraaij – Dirkzwager ()1, A Timen1, K Dirksen2, L Gelinck3, E Leyten3, P Groeneveld4, C Jansen3, M Jonges5, S Raj6, I Thurkow7, R van Gageldonk-Lafeber8, A van der Eijk6, M Koopmans5,6, on behalf of the MERS-CoV outbreak investigation team of the Netherlands9
Citation style for this article: Kraaij – Dirkzwager M, Timen A, Dirksen K, Gelinck L, Leyten E, Groeneveld P, Jansen C, Jonges M, Raj S, Thurkow I, van Gageldonk-Lafeber R, van der Eijk A, Koopmans M, on behalf of the MERS-CoV outbreak investigation team of the Netherlands. Middle East respiratory syndrome coronavirus (MERS-CoV) infections in two returning travellers in the Netherlands, May 2014. Euro Surveill. 2014;19(21):pii=20817. Available online: http://www.eurosurveillance.org/ViewArticle.aspx?ArticleId=20817
Date of submission: 21 May 2014
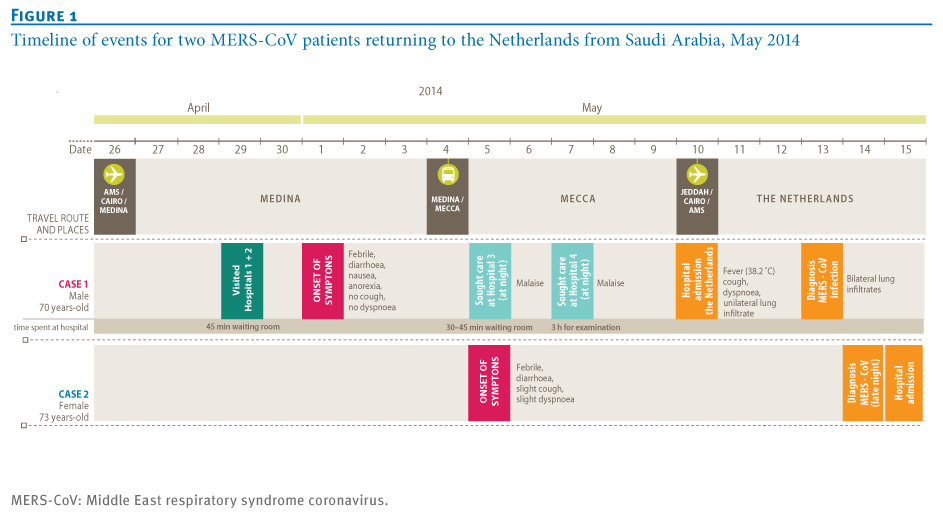
Two patients, returning to the Netherlands from pilgrimage in Medina and Mecca, Kingdom of Saudi Arabia, were diagnosed with Middle East respiratory syndrome coronavirus (MERS-CoV) infection in May 2014. The source and mode of transmission have not yet been determined. Hospital-acquired infection and community-acquired infection are both possible.
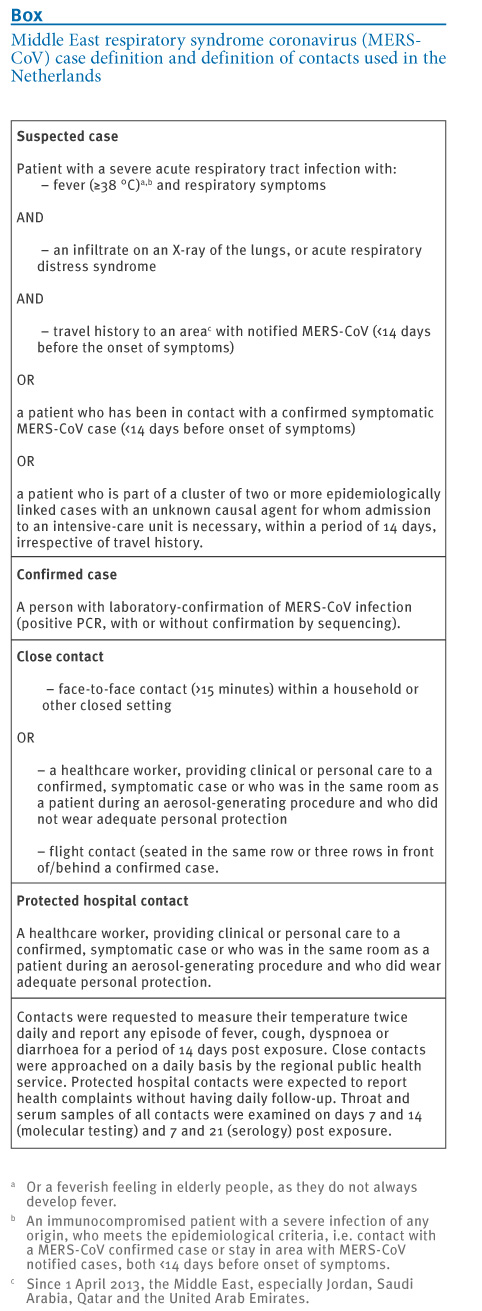
On 13 May 2014, a Dutch patient, returning to the Netherlands from pilgrimage in Medina and Mecca, Kingdom of Saudia Arabia, was diagnosed with Middle East respiratory syndrome coronavirus (MERS-CoV) infection, followed by diagnosis of a second patient, belonging to the same tour group, the day after. Here we describe the two cases and the public health response. The case definition that is used in the Netherlands is outlined in the Box.
<BIG SNIP>
Discussion
There are several options for the possible source of the infection of the two Dutch cases: Case 1 could have been infected during the hospital visit of his child on 29 April, after which he infected Case 2. Alternatively, both could have been exposed to a common, as yet unknown, source in Medina. Thirdly, each case could have been infected through different sources (hospital/ community), though this seems unlikely, as the (partial) virus sequence of both cases was nearly identical.
The resemblance in strain sequence between the Dutch cases and the case from the US is remarkable as the cases did not visit the same places in the Kingdom of Saudi Arabia. Exchange of information between the US Centers for Disease Control and Prevention and Dutch experts did not reveal any clues about mutual exposure of the Dutch and US cases.
The current, limited scientific information does not support any conclusion on the meaning of this genetic resemblance, knowing that multiple lineages of the virus can be found in camels and people [2,12]. Continued vigilance in evaluation of contacts of imported cases, including molecular testing and serology, will hopefully lead to better insights.
{kind=link}
{kind=link}