#13,812
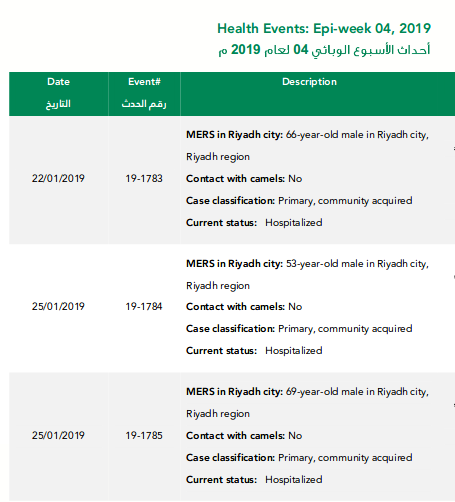
This morning the Saudi MOH announced 2 more community acquired MERS cases in Riyadh, making four such cases in the capital city in the past 6 days (see previous posts here, and here).
All patients are male (ages 40, 66, 53 & 69), are hospitalized (condition not stated), and are listed as primary, community acquired with no camel contact.Today's Epi Week 4 update reads:
Direct or indirect camel contact is often cited as a source of MERS infection - along with contact with a known MERS case (usually in a household or hospital cluster) - but in roughly half the cases the source of infection is never identified.
Community acquired cases simply turn up, leaving how and where they acquired the virus a mystery. There are strong suspicions, however, that mildly ill - or potentially asymptomatic cases - in the community are spreading the virus, albeit inefficiently.While the official case count stands (as of Dec 31st) at 2279 laboratory-confirmed cases and 806 deaths globally, the true burden of this disease remains unknown. Since shortly after the virus emerged in 2012, we've seen analyses that have concluded that only a fraction of MERS cases are likely diagnosed, including:
- In November of 2013, we looked at a study published in The Lancet Infectious Diseases, that estimated for every case identified, there are likely 5 to 10 that go undetected.
- In 2015, when Saudi Arabia had recorded fewer than 1200 MERS cases, a seroprevalence study (see Presence of Middle East respiratory syndrome coronavirus antibodies in Saudi Arabia: a nationwide, cross-sectional, serological study by Drosten & Memish et al.,) suggested nearly 45,000 might have been infected.
- And a 2016 study (see EID Journal: Estimation of Severe MERS Cases in the Middle East, 2012–2016) suggested that as much as 60% of severe Saudi MERS cases go undiagnosed.
J. Korean Med Sci: Atypical Presentation Of A MERS Case In A Returning Traveler From KuwaitLast August - in Evaluation of a Visual Triage for the Screening of MERS-CoV Patients - we also looked at what has been described as a serious flaw in Saudi Arabia's MERS surveillance program.
mBio: High Prevalence of MERS-CoV Infection in Camel Workers in Saudi Arabia
AJIC:Intermittent Positive Testing For MERS-CoV
JIDC: Atypical Presentation Of MERS-CoV In A Lebanese Patient
A 2017 study (see A Pandemic Risk Assessment Of MERS-CoV In Saudi Arabia) provided a detailed statistical analysis of MERS-COV cases reported in Saudi Arabia from May 2013 to May 2015.
The yardstick by which disease transmissibility is measured is its R0 (pronounced R-nought) or Basic Reproductive Number. Essentially, the number of new cases in a susceptible population likely to arise from a single infection.
In the simplest of terms, with an R0 below 1.0, a virus (as an outbreak) begins to sputter and dies out. Above 1.0, and an outbreak can have `legs’.That Pandemic Risk Assessment calculated an R0 (R: 0.85–0.97) across all regions, but found in central and western regions that at times the R0 flirted with epidemic sustaining numbers.
While the number of community MERS cases remains limited, we watch these reports with the knowledge that we are probably only seeing the tip of the iceberg, and remain alert to any potential changes in the way the virus transmits in the community.