#16,061
After delaying their decision for a month - as expected - last night the UK Prime Minister Boris Johnson confirmed that six days from now nearly all legal restrictions on social contact will end (see BBC report Covid: England lockdown rules to end on 19 July, PM confirms).
This policy change comes, in large part, due to a growing dissatisfaction of the public after 18 months of COVID restrictions, and a need to reinvigorate a flagging economy. But it also comes with no small amount of risk.
Yesterday, while supportive of this change, their new Health Secretary Sajid Javid warned Parliament of a potential tripling of cases by the end of summer due to the Delta variant (see excerpts from statement below).
Mr Speaker, our third test is around whether infection rates would put unsustainable pressure on the NHS. And I want to be open about what the data is telling us, and why we’ve reached the decision we have.
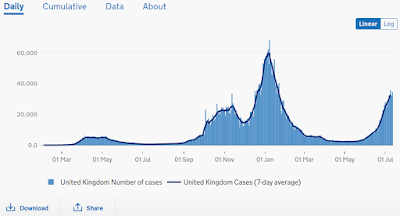
Cases are rising, propelled by the new, more transmissible Delta variant. The average number of daily new cases is over 26,000 and this has doubled over the past 11 days. And sadly, the case numbers will get a lot worse before they get better. We could reach 100,000 cases a day later in the summer.
Hospitalisations are also rising, with sustained growth over the past month – and once again, they will rise too. But we should be encouraged that hospitalisations are far lower than they were at this point during the previous wave.
Just as we should be encouraged that people over 65 who are more likely to have had both doses of a vaccine make up 31 per cent of Covid admissions in the last week, compared to 61 per cent in January.
This is further evidence that our vaccination programme is doing its job and protecting our NHS. And as more people get the jab, our protective wall will get stronger still.
We will stay vigilant and keep a close eye on the data, as well as the impact of long-COVID, where we’re investing £50 million into research.
But on the basis of the evidence in front of us, we do not believe that infection rates will put unsustainable pressure on the NHS. It’s so important that everyone does their bit in helping the NHS to stand strong.
The gamble is that while cases will rise - potentially even higher than last winter - that due to the impact of the vaccine, and its high uptake among the most vulnerable population, that most cases will be mild, and the surge will be manageable.
The UK's decision comes despite the risk assessment issued by the ECDC two weeks ago (see Threat Assessment On Spread of COVID Variant B.1.617.2 (Delta) VOC) which bluntly warned against relaxation of nonpharmaceutical measures to reduce the spread of the Delta variant, and another from the WHO that urged fully vaccinated people to continue to wear face masks.Of course, there are other possible pitfalls; including the impact of `Long COVID' among those with mild illness, the potential for additional variants to emerge, and a very real possibility of a `twindemic' of influenza and other respiratory viruses alongside COVID this fall and winter.
Yesterday Imperial College London released their analysis of the likely fallout from removing all COVID restrictions - and while they don't settle on one outcome - they do provide a range (from optimistic to more pessimistic) of likely results.
Evaluating the Roadmap out of Lockdown for England: modelling the delayed step 4 of the roadmap in the context of the Delta variant
Raphael Sonabend, Natsuko Imai, Edward S Knock, Pablo N Perez-Guzman, Lilith K Whittles, Thomas Rawson, Tara Mangal, Erik M Volz, Neil M Ferguson, Marc Baguelin, Anne Cori
MRC Centre for Global Infectious Disease Analysis, Imperial College London1. Summary This report summarises the findings of our evaluation of the easing of non-pharmaceutical interventions (NPIs) set out in the UK Government’s Roadmap out of Lockdown, focusing on the delayed step 4 of the roadmap and the potential impact of the Delta variant (B.1.617.2). Full methods, data used, and parameter values assumed for forward projections are given in the technical appendix. Key parameters relevant to interpretation of findings are provided in the text. 1. Based on Public Health England (PHE) data available to 2 July 2021, 84% of the adult population in England have received one vaccine dose and 62% have received two doses.2. Across all transmissibility and vaccine effectiveness (VE) scenarios explored, we estimate that lifting restrictions on 19 July in the context of Delta could lead to a significant third wave of hospitalisations and deaths.3. The projected scale of the third wave is highly sensitive to small changes in assumptions about vaccine effectiveness. It is also sensitive to the assumed reproduction number of Delta following Step 4.4. Under optimistic assumptions for both, the third wave is likely to lead to substantially lower numbers of hospitalisations and deaths than seen in the second wave last winter.5. However, under more pessimistic assumptions, hospitalisations and deaths in the third wave could substantially exceed those seen in the second wave.6. Our central scenarios suggest hospitalisation numbers comparable with, but deaths substantially lower than, the second wave.7. If population contact rates only increase gradually between 19th July and 1st September, the third wave will be both delayed and reduced in size compared with a scenario where there is an abrupt change in contact rates following Step 4.8. In comparison, delaying step 4 until 16 August with a sharp increase in transmissibility at that point, delays the third wave but has less of an impact on peak hospitalisations or total deaths.9. Emphasis on, and good adherence to, baseline NPIs after 19 July may therefore play an important role in reducing hospitalisations and deaths as it could dampen and slow the increase in (potentially infectious) contact rates in the population.10.There is considerable uncertainty regarding i) the levels of cross protection against Delta from prior infection with other variants; ii) the proportion of vaccine failure against Delta for severe outcomes (known to be small but unclear how small); and iii) the level of transmission after NPIs are lifted. This translates into large uncertainty in the possible future epidemic trajectory.
(SNIP)
4. Conclusions
Our results highlight the large uncertainty regarding both the level of cross protection and vaccine effectiveness against Delta as well as the transmissibility after NPIs are lifted at step 4. This translates into large uncertainty on the possible future epidemic trajectory. However, all scenarios considered resulted in a substantial third wave of infections and hospitalisations. If adherence to current step 3 measures wanes gradually over the summer (rather than a sudden increase in transmissibility on 19 July), then the wave of hospitalisations and deaths can be substantially reduced and delayed.
Therefore, whilst the impact of Test Trace Isolate (TTI), mask wearing, hand hygiene, and COVID security on R is difficult to quantify, it will be vital to emphasise the importance of normalising and ensuring adherence to all measures even after “full lifting” is achieved. For both scenarios where step 4 is delayed, or there is a gradual waning in adherence to step 3 measures, the projected third wave is delayed, allowing more time for further mitigating measures such as booster doses to be implemented.
Given the large uncertainty regarding the possible magnitude of the future wave, continuous careful monitoring of the epidemic trajectory will be critical as will further evidence on vaccine effectiveness against the Delta variant.
Preventing the further importation and spread of variants of concerns (VOC) with moderate to high immune escape properties will be critical as these could lead to future waves orders of magnitude larger than the ones experienced so far.
While there are considerable risks in the field experiment the UK is about to conduct, they are probably one of the better equipped countries - due to having both universal health care and unparalleled testing and sequencing capacity - to attempt it.
If they succeed, they could provide valuable information and a roadmap for other countries to follow in the months ahead. If things go less swimmingly, they could serve as a warning to others not to proceed as boldly.
Either way, the world will be watching with great interest.