
#17,609
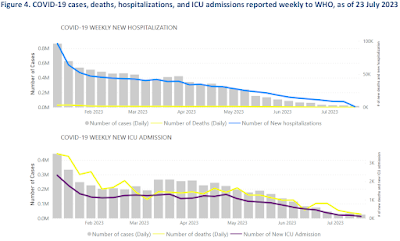
Based on what is being reported by countries around the world, one could be forgiven for believing that COVID was all but over. The WHO's latest report (update on COVID-19 - 3 August 2023) shows that reported hospitalizations, and ICU admissions, have plummeted since last winter.
But there is an asterisk attached. A very big one in fact.
Only about 7% of member nations regularly reported data in the past 28 days (see chart below). A percentage that has been steadily dwindling for months.

Most of what we know comes from scaled-back reporting from a handful of (mostly) European nations. Which is why you'll find some pretty broad disclaimers throughout this report, including:
- Note: Recent weeks are subject to reporting delays and data might not be complete, note to interpret the data with caution. Cases included in grey bars in the graph are only from countries reporting hospitalizations or ICU admissions, respectively.
- Note: Recent weeks are subject to reporting delays and should not be interpreted as a declining trend.
- `sustain collaborative surveillance for COVID-19'
- and to `continue reporting COVID-19 data, particularly mortality data, morbidity data, SARS-CoV-2 genetic sequences with meta-data, and vaccine effectiveness data to WHO'.
Whether there is enough political will to make any of that happen remains to be seen. But at the same time the WHO was releasing this appeal, they also released an initial risk assessment on the EG.5 COVID variant, which has been making strides in a number of countries around the world.
While barely a blip on the CDC's Nowcast 6 weeks ago, EG.5 pulled ahead of XBB.1.16 last week, and it (and FL.1.5.1) continues to show the most signs of growth.

Although hampered by the limited surveillance and reporting from > 90% of member nations, the WHO has elevated EG.5 from being a Variant Under Monitoring (VUM) to being a (VOI) Variant of Interest.
For now, based on admittedly limited data, the WHO sets the Global Public Health Risk to Low.
Some excerpts from the 5-page report follow. Click the link to read it in its entirety.
EG.5 Initial Risk Evaluation, 9 August 2023
EG.5 is a descendent lineage of XBB.1.9.2, which has the same spike amino acid profile as XBB.1.5. EG.5 was first reported on 17 February 2023, and designated as a variant under monitoring (VUM) on 19 July 2023. With this risk evaluation, we are designating EG.5 and its sub-lineages as a variant of interest (VOI).
EG.5 carries an additional F456L amino acid mutation in the spike protein compared to the parent XBB.1.9.2 subvariant and XBB.1.5. Within the EG.5 lineage, the subvariant EG.5.1 has an additional spike mutation Q52H and represents 88% of the available sequences for EG.5 and its descendent lineages.
As of 7 August 2023, 7354 sequences of EG.5 have been submitted to GISAID from 51 countries. The largest portion of EG.5 sequences are from China (30.6%, 2247 sequences). The other countries with at least 100 sequences are the United States of America (18.4%, 1356 sequences), the Republic of Korea (14.1%, 1040 sequences), Japan (11.1%, 814 sequences), Canada (5.3%, 392 sequences), Australia (2.1%, 158 sequences), Singapore (2.1%, 154 sequences), the United Kingdom (2.0%, 150 sequences), France (1.6%,119 sequences), Portugal (1.6%, 115 sequences), and Spain (1.5%, 107 sequences).
Globally, there has been a steady increase in the proportion of EG.5 reported. During epidemiological week 29 (17 to 23 July 2023), the global prevalence of EG.5 was 17.4%. This is a notable rise from the data reported four weeks prior (week 25, 19 to 25 June 2023), when the global prevalence of EG.5 was 7.6%.
Based on the available evidence, the public health risk posed by EG.5 is evaluated as low at the global level, aligning with the risk associated with XBB.1.16 and the other currently circulating VOIs (see risk evaluation table below). While EG.5 has shown increased prevalence, growth advantage, and immune escape properties, there have been no reported changes in disease severity to date.
While concurrent increases in the proportion of EG.5 and COVID-19 hospitalizations (lower than previous waves) have been observed in countries such as Japan and the Republic of Korea, no associations have been made between these hospitalizations and EG.5. However, due to its growth advantage and immune escape characteristics, EG.5 may cause a rise in case incidence and become dominant in some countries or even globally.
WHO and its Technical Advisory Group on SARS-CoV-2 Evolution (TAG-VE) continue to recommend that Member States prioritize specific actions to better address uncertainties relating to antibody escape and severity of EG.5. The suggested timelines are estimates and will vary from one country to another based on national capacities:
• Share information on the growth advantage of EG.5 in your country and/or provide sequence information (1-4 weeks).
• Conduct neutralization assays using human sera, representative of the affected community(ies), and EG.5 live virus isolates (2-4 weeks, see table below for the results from previously conducted).
• Perform a comparative evaluation to detect changes in rolling or ad hoc indicators of severity (4-12 weeks, see table below for the results from previously conducted studies).
The WHO and its Technical Advisory Group on COVID-19 Vaccine Composition (TAG-CO-VAC) continue to regularly assess the impact of variants on the performance of COVID-19 vaccines to inform decisions on updates to vaccine composition.(2) The risk evaluation below is based on currently available evidence and will be revised regularly as more evidence and data from additional countries become available.
Amongst the VOIs and VUMs featuring the F456L mutation and for the period 19 June to 23 July 2023, EG.5 is most reported at 49.1%, compared to other VOI and VUM including XBB.1.16.6 (4.88%), FL.1.5.1 (4.41%), XBB.1.5.10 (4.06%), XBB.1.5.72 (3.52%), EG.6.1 (3.26%), FD.1.1 (3.07%), EG.5.2 (3.06%), FE.1.1 (2.58%), FL.15 (2.47%), FE.1.2 (2.09%), XBB.1.5.70 (1.91%), GK.1 (1.83%), FE.1.1.1 (1.68%), XBB.1.5.59 (1.31%), XBB.1.5 (1.27%), GN.1 (1.26%), XBB.1.16.9 (1.15%), FL.1.5 (1.08%), and XBB.1.9.1 (1.07%), among others with reported prevalence less than one percent.


Right now there are no obvious warning signals suggesting that EG.5 will be any worse than any of the previous Omicron strains of the past year. It will likely drive a new wave of (mostly mild) infections, but hopefully nothing worse.
But the lack of global surveillance and reporting make risk assessments like this difficult, and for 2 of the 3 indicator categories (antibody escape & severity), the WHO's confidence level is low.
So surprises are always possible.
Far more dangerous in the long run, however, is our willingness to wear blinders when reporting on emerging infectious diseases. EG.5 may not become the next big health crisis, but somewhere out there, the next contender is lurking.
And it would be far better if we find it, before it finds us.