
Credit Eurosurveillance
# 7253
From the Eurosurveillance Journal today, a Rapid Communications that examines the H7N9 outbreak in China, and attempts to gauge the relative seriousness of the infection in the elderly versus younger adults, and the likely minimum spread of the disease (in humans) to date.
Using data from two unpublished surveys of individual poultry exposures conducted in Guangdong and Anhui province several years ago, they then used the demographics of first 102 known cases to model the outbreak.
In doing so, they had to make two major assumptions:
- The risk of infection was directly proportional to the risk of exposure
- The seriousness of infection varied by age.
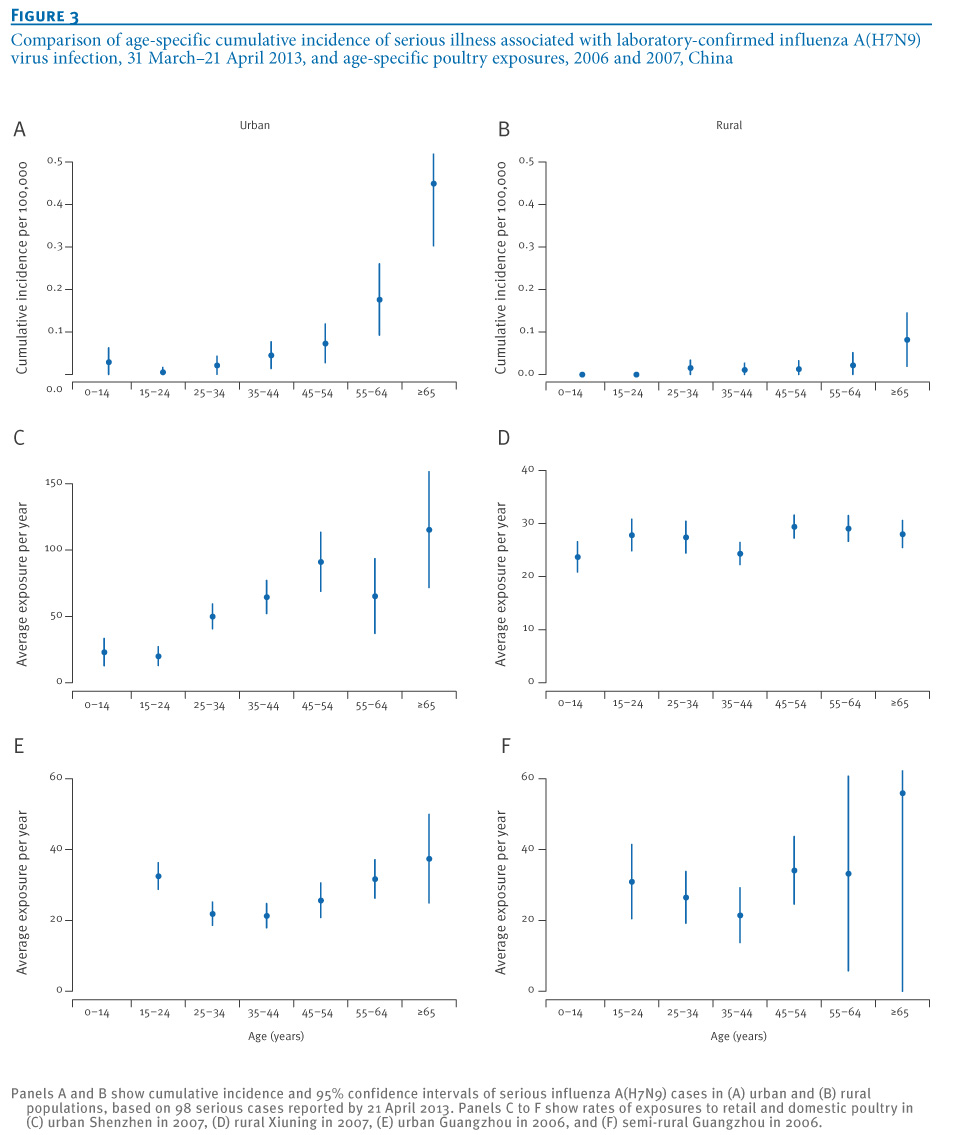
Using statistical analysis techniques that are well and truly above my pay grade, they calculated a minimum 5.06-fold increase (95% CI: 2.99–8.15) in the risk of serious illness for those aged 65 years and older and an estimated minimum 352 (95% CI: 225–541) H7N9 infections.
First a link to the study, then I’ll return with more.
Eurosurveillance, Volume 1
8, Issue 19, 09 May 2013
Rapid communications
B J Cowling , G Freeman, J Y Wong, P Wu, Q Liao, E H Lau, J T Wu, R Fielding, G M Leung
Citation style for this article: Cowling BJ, Freeman G, Wong JY, Wu P, Liao Q, Lau EH, Wu JT, Fielding R, Leung GM. Preliminary inferences on the age-specific seriousness of human disease caused by avian influenza A(H7N9) infections in China, March to April 2013 . Euro Surveill. 2013;18(19):pii=20475.
Date of submission: 25 April 2013
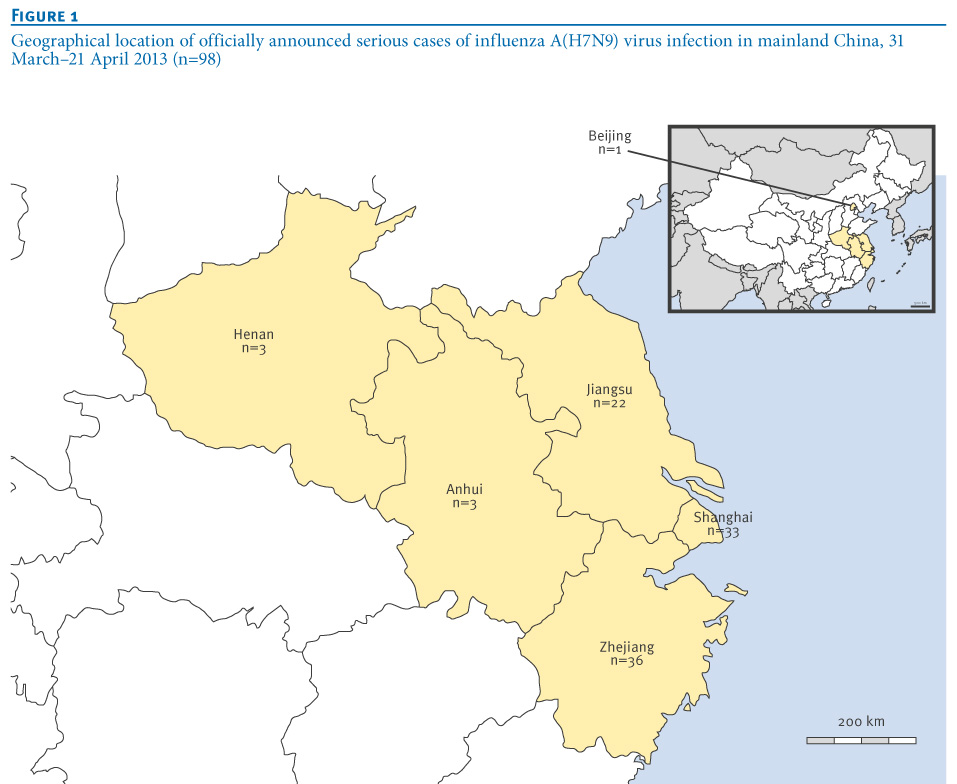
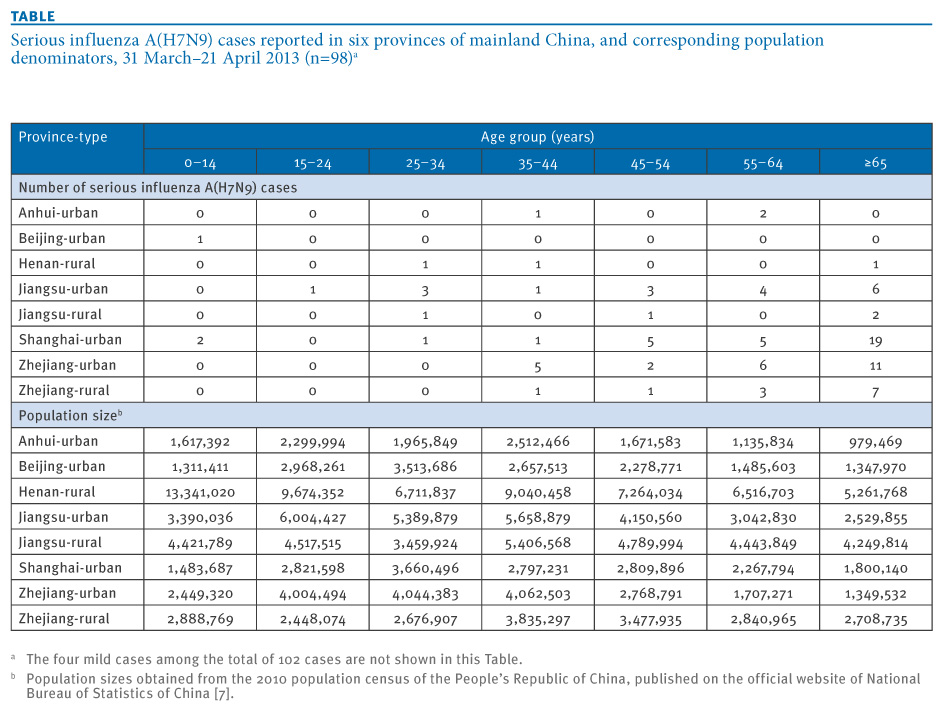
Between 31 March and 21 April 2013, 102 laboratory-confirmed influenza A(H7N9) infections have been reported in six provinces of China. Using survey data on age-specific rates of exposure to live poultry in China, we estimated that risk of serious illness after infection is 5.1 times higher in persons 65 years and older versus younger ages.
Our results suggest that many unidentified mild influenza A(H7N9) infections may have occurred, with a lower bound of 210–550 infections to date.
{kind=link}
{kind=link}
{kind=link}
You may recall that back on April 22nd (see H7N9: Trying To Define The Size Of The Iceberg) we saw an interview by the corresponding author of this paper, B J Cowling, where he estimated the number of cases at roughly double the laboratory confirmed numbers.
Figuring out how many mild, or asymptomatic cases have occurred is important, both to helping to determine how the virus might be spreading, and to fine tune its CFR – or Case Fatality Ratio.
Based on known (laboratory confirmed) cases, the CFR sits near 20%, a devastatingly high mortality rate for any influenza.

The chart above (courtesy of Ian Mackay’s VDU H7N9 website) illustrates this `apparent CFR’. Ian discusses the `denominator problem’, and how it affects the CFR on his site.
If we assume that the estimates in today’s study are correct - and there are at least three times as many cases out there than we know about - then the CFR would drop well into the single digits.
Still a formidable fatality rate, by any measure.
The authors of this study readily admit that there are limitations to this type of statistical modeling. They write:
Our estimates are limited by the lack of data on exposures in affected urban and rural areas. In particular, the higher risk for infection in males compared to females could be due to variation in sex-specific rates of exposure by region [5]. Without data on such differences, we did not include sex in our models.
Most confirmed cases report exposure to live poultry [3] and this remains the most likely source of infection for the majority of influenza A(H7N9) cases. However, the exposure distributions used in our analysis may not fully capture the age-specific risk profile, if there are other sources of infection apart from retail and domestic poultry. As of April 25, we are not aware of provinces in China with laboratory-confirmed A(H7N9) cases in poultry but not in humans.
Finally, no published information is available on population levels of immunity to influenza A(H7N9), although preliminary investigations suggest very low antibody levels against influenza A(H7N9) virus in all ages, and we assumed there was no heterogeneity in immunity by age. If older persons had some degree of immunity against influenza A(H7N9) through potential past exposures to avian influenza viruses, this would imply an even higher number of undetected infections in adults based on our method.
In conclusion, we estimated a lower bound for the number of influenza A(H7N9) infections based on the possible age distribution of exposures and varying seriousness of infection by age. More accurate estimates of the risk of influenza A(H7N9) infection and the age-specific seriousness of infection could be provided by detailed seroepidemiological studies in affected areas [15].
In the end, we really won’t have a really good handle on the real attack rate of this virus until seroprevalence studies can be conducted across multiple locations.
But until that can happen, statistical modeling such as this can give us some sense of what is out there that we currently cannot count.