
{kind=link}
# 8150
While it’s not easy to find anything good to say about a pandemic influenza virus, the 2009 pH1N1 strain had at least one saving grace; unlike the old seasonal H1N1 strain it replaced, it was overwhelming sensitive to Neuraminidase Inhibitor (NAI) antiviral drugs like oseltamivir (Tamiflu ®) and zanamivir (Relenza ®).
In 2006 we only saw a smattering of oseltamivir resistant seasonal H1N1 cases, almost always attributed to `spontaneous mutations’ within a patient receiving the drug. While of concern to the patient being treated, it appeared to be poorly transmissible.
In the 2006-2007 flu season, laboratories found no resistant strains in Europe or Japan, and in less than 1% of samples from the United States.
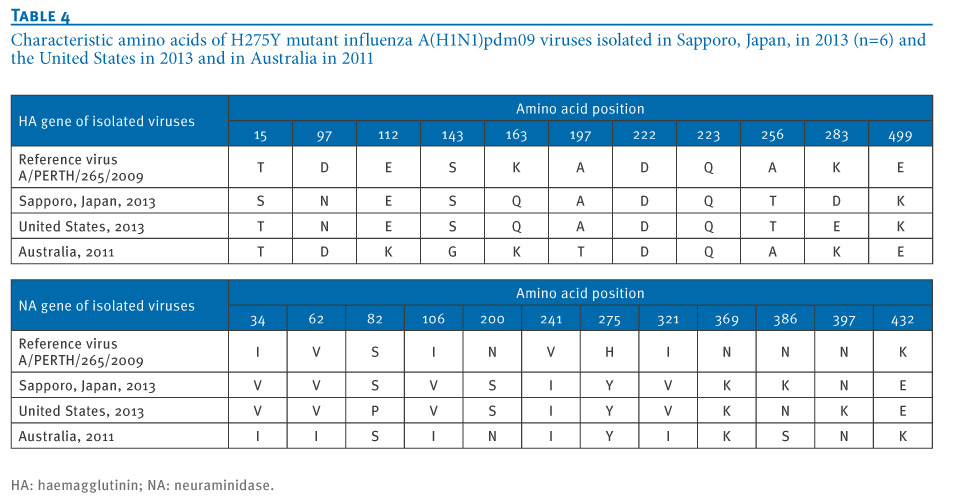
Resistance in this viral strain was mostly caused by a mutation called H275Y, where a single amino acid substitution (histidine (H) to tyrosine (Y)) occurs at the neuraminidase position 275.
(Note: some scientists use 'N2 numbering' (H274Y) and some use 'N1 numbering' (H275Y))
The following year, during the 2007-2008 flu season, oseltamivir resistant viruses suddenly took flight, and by the spring of 2008 roughly 25% of European samples tested showed the H275Y mutation (see Increased Tamiflu Resistance In Seasonal Influenza).
By December of 2008 nearly all of the samples tested in the United States were resistant to oseltamivir and the CDC was forced to issue major new guidance for the use of antivirals (see CIDRAP article With H1N1 resistance, CDC changes advice on flu drugs).
The arrival of a the pandemic H1N1 in the spring of 2009 effectively removed this resistant strain from circulation, and in the five ensuing years, nearly 99% of the pH1N1 viruses tested have remained sensitive to NA inhibiting drugs. The latest FluView report (week 52) indicated that of 910 viruses tested, only 10 showed signs of NA Inhibitor resistance.

While 99% sensitivity is an excellent batting average in any league, 5 of the 10 resistant viruses were detected in Louisiana and Mississippi, suggesting a geographic clustering of cases.
Although we have seen some signs the pH1N1 might be figuring its way around our arsenal of antivirals, most often this occurs after a patient is placed on antivirals, occasionally resulting in a spontaneous mutation within the host.
But we have seen some signs of community spread of resistant pH1N1 as well.
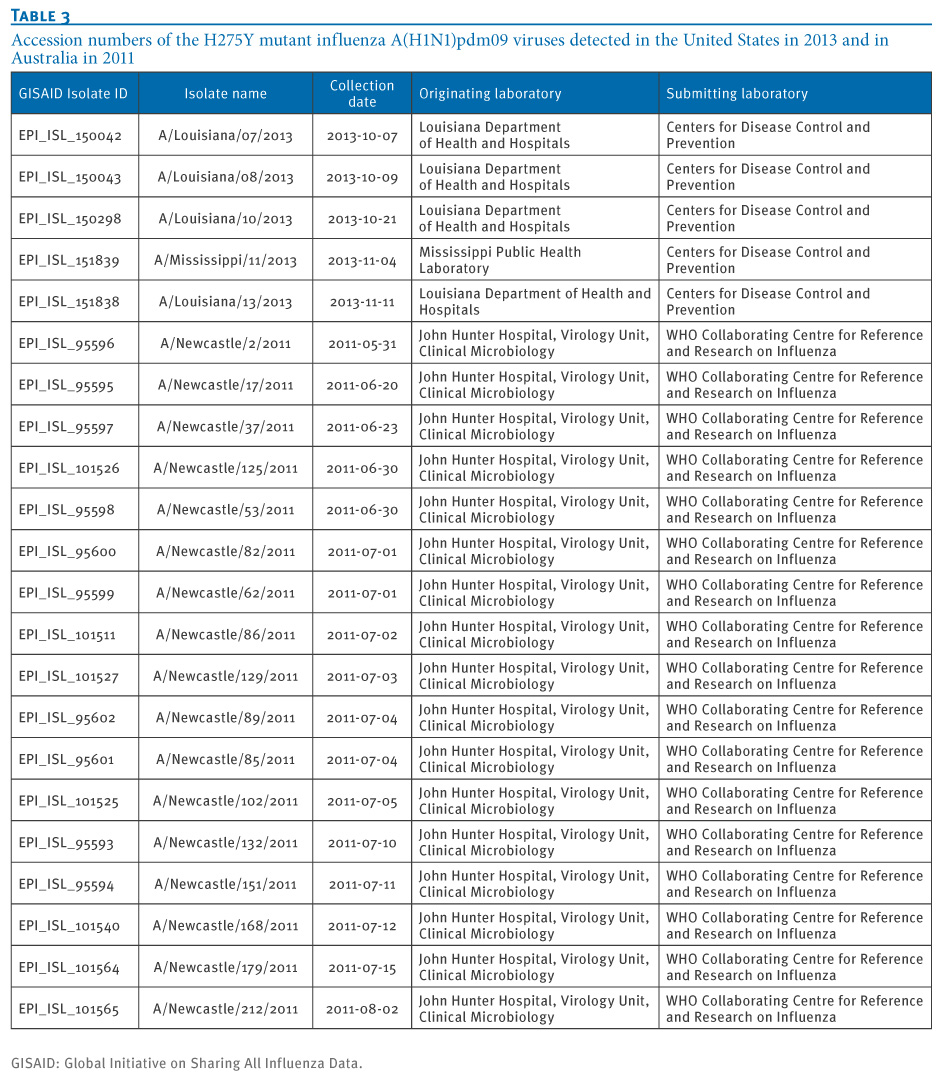
Readers with good memories will recall that in December of 2011, in NEJM: Oseltamivir Resistant H1N1 in Australia, we looked at a cluster of oseltamivir (Tamiflu ®) resistant H1N1 viruses in and around the Newcastle area of New South Wales.
The lead author of that NEJM correspondence was Aeron C. Hurt, Ph.D. from the World Health Organization (WHO) Collaborating Centre for Reference and Research on Influenza, North Melbourne, VIC, Australia.
What Hurt and his colleagues found was evidence for the sustained community transmission of a resistant strain of the H1N1pdm09 virus.
After analyzing viral samples pulled from 182 patients seen in emergency departments, intensive care units, and doctor’s offices in New South Wales between May and August of 2011, they found 29 (16%) carried the H275Y resistance mutation.
In 2011, we also saw reports of a `mildly resistant’ version of pH1N1 – with a different mutation S247N (serine (S) to asparagine (N)) mutation at the neuraminidase position 247) – showing up with some frequency in Australia, Brunei and Singapore (see Eurosurveillance: A `Mildly’ Resistant Strain of H1N1 Emerges).
But neither of these strains has gained much traction globally, and the World Health Organization still reports only about 2% of samples tested are resistant to our frontline antiviral drugs.
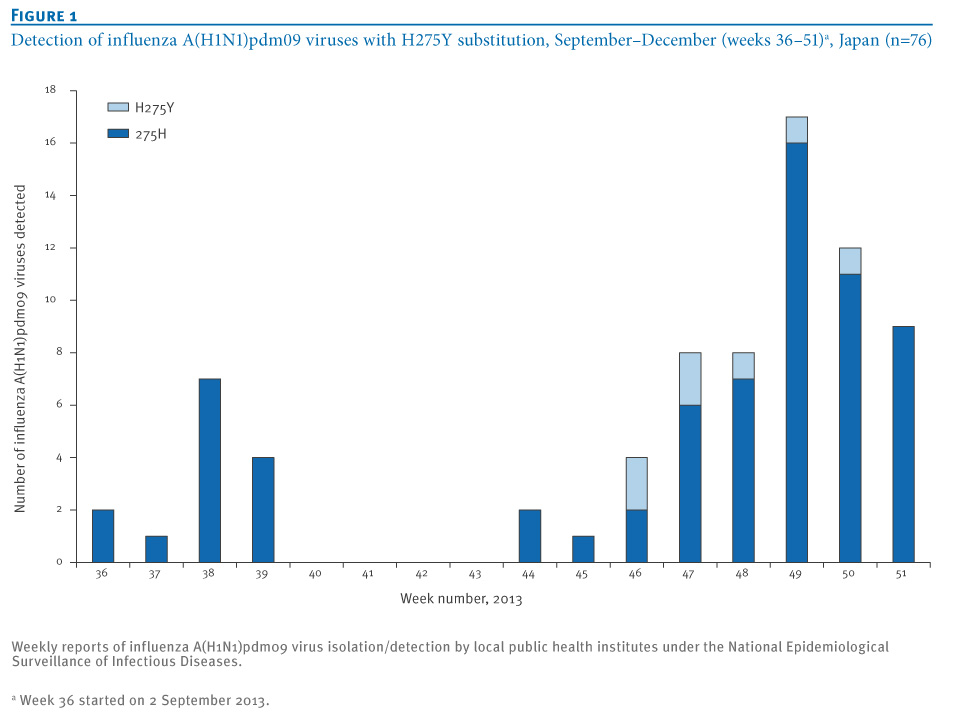
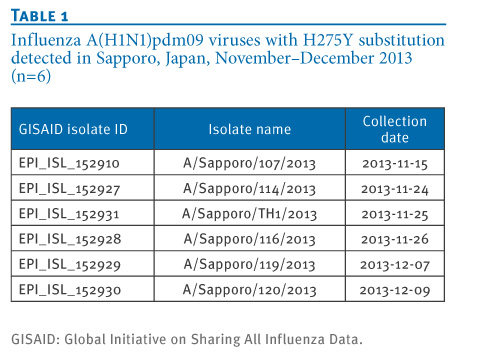
Today, we’ve a Rapid Communications in the journal Eurosurveillance that details a recent community cluster of resistant pH1N1 (with the H275Y mutation) in Sapporo, Japan. Six genetically similar viruses were detected, although none of the patients had known contact with each other, which suggests a resistant strain may be starting to spread in that region.
Rapid communications
E Takashita1, K Ejima1, R Itoh1, M Miura1, A Ohnishi2, H Nishimura3, T Odagiri1, M Tashiro (
)1
- Influenza Virus Research Center, National Institute of Infectious Diseases, Tokyo, Japan
- Sapporo City Institute of Public Health, Hokkaido, Japan
- Virus Research Center, Sendai Medical Center, Miyagi, Japan
Citation style for this article: Takashita E, Ejima K, Itoh R, Miura M, Ohnishi A, Nishimura H, Odagiri T, Tashiro M. A community cluster of influenza A(H1N1)pdm09 virus exhibiting cross-resistance to oseltamivir and peramivir in Japan, November to December 2013. Euro Surveill. 2014;19(1):pii=20666. Available online: http://www.eurosurveillance.org/ViewArticle.aspx?ArticleId=20666
Date of submission: 30 December 2013
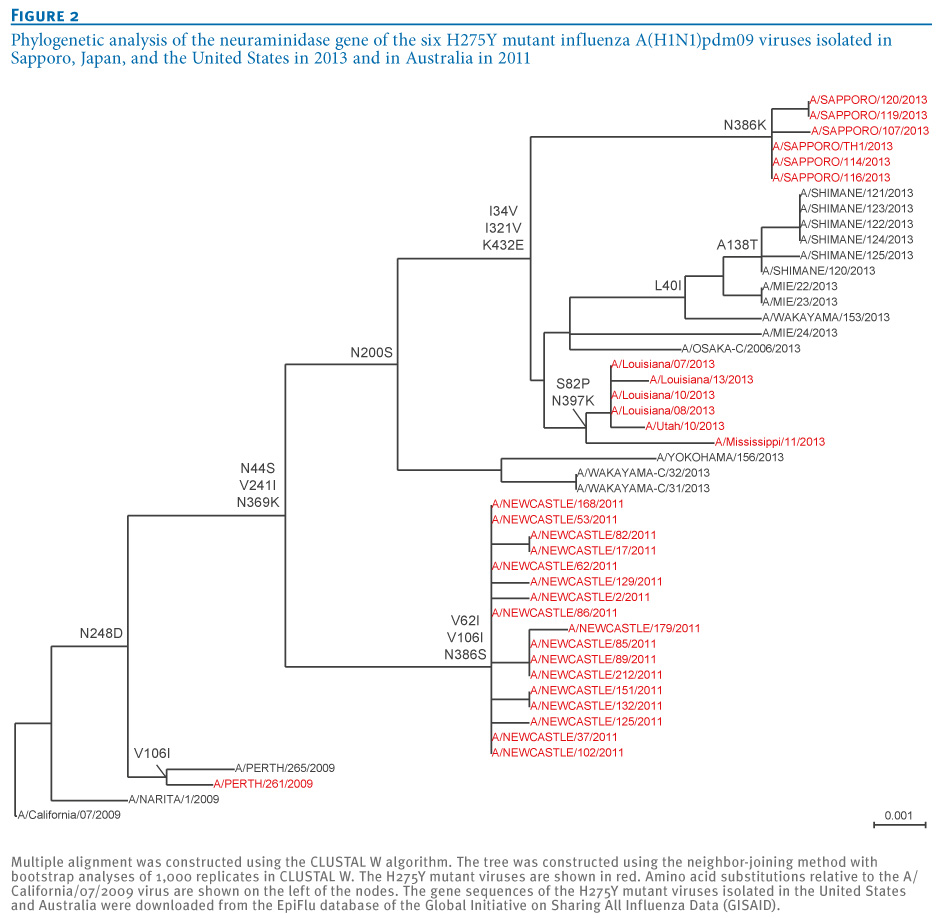
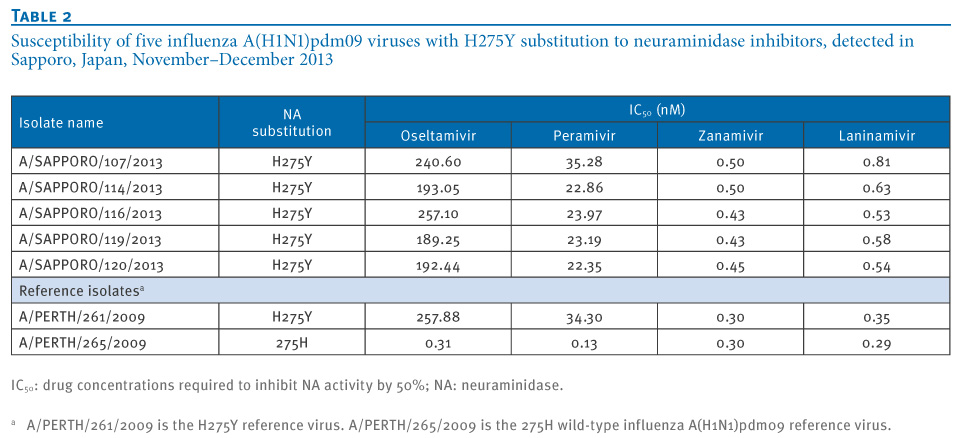
Six influenza A(H1N1)pdm09 viruses were detected in Sapporo, Japan, between November and December 2013. All six viruses possessed an H275Y substitution in the neuraminidase protein, which confers cross-resistance to oseltamivir and peramivir. No epidemiological link among the six cases could be identified; none of them had received neuraminidase inhibitors before specimen collection. The haemagglutinin and neuraminidase genes of the six viruses were closely related to one another, suggesting clonal spread of a single resistant virus.
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
In their discussion, the authors write:
It has been shown that oseltamivir-resistant influenza A(H1N1) virus infection reduced the effectiveness of oseltamivir and this tendency was more apparent in children 0 to 6 years old [14-16]. Among patients from whom oseltamivir- and peramivir-resistant A(H1N1)pdm09 viruses have been detected in Japan, the percentage with no known exposure to NA inhibitors has increased significantly, from 16% during the pandemic period to 44% during the post-pandemic period [2]. These observations may suggest that human-to-human transmission with H275Y mutant viruses has increased gradually in the post-pandemic period. Consequently, surveillance of antiviral-resistant influenza viruses should be continued and strengthened, particularly for the choice of antiviral drugs.
Since 2009 we’ve seen sporadic cases of antiviral resistance show up in the new H1N1 virus, but only rarely have we seen clusters that suggest limited community spread. So we are nowhere near the level of concern over antiviral resistance that we experienced in 2008.
That said, we know that pharmacological victories over viruses and bacteria have always been fleeting at best. Pathogens – given enough time – have demonstrated a keen ability to evade each new generation of drugs we throw at them.
A reminder that in our ongoing battle against infectious diseases, that nature always bats last.