#10,845
The Overseas Security Advisory Council (OSAC), a department within the United States Department of State, has issued an adivsory on the growing Zika epidemic in Brazil for all American citizens visiting that country.
With Carnival in Rio just over a month away, and the summer Olympics scheduled for next August, the recent introduction and rapid spread of Zika in Brazil takes on even greater importance.
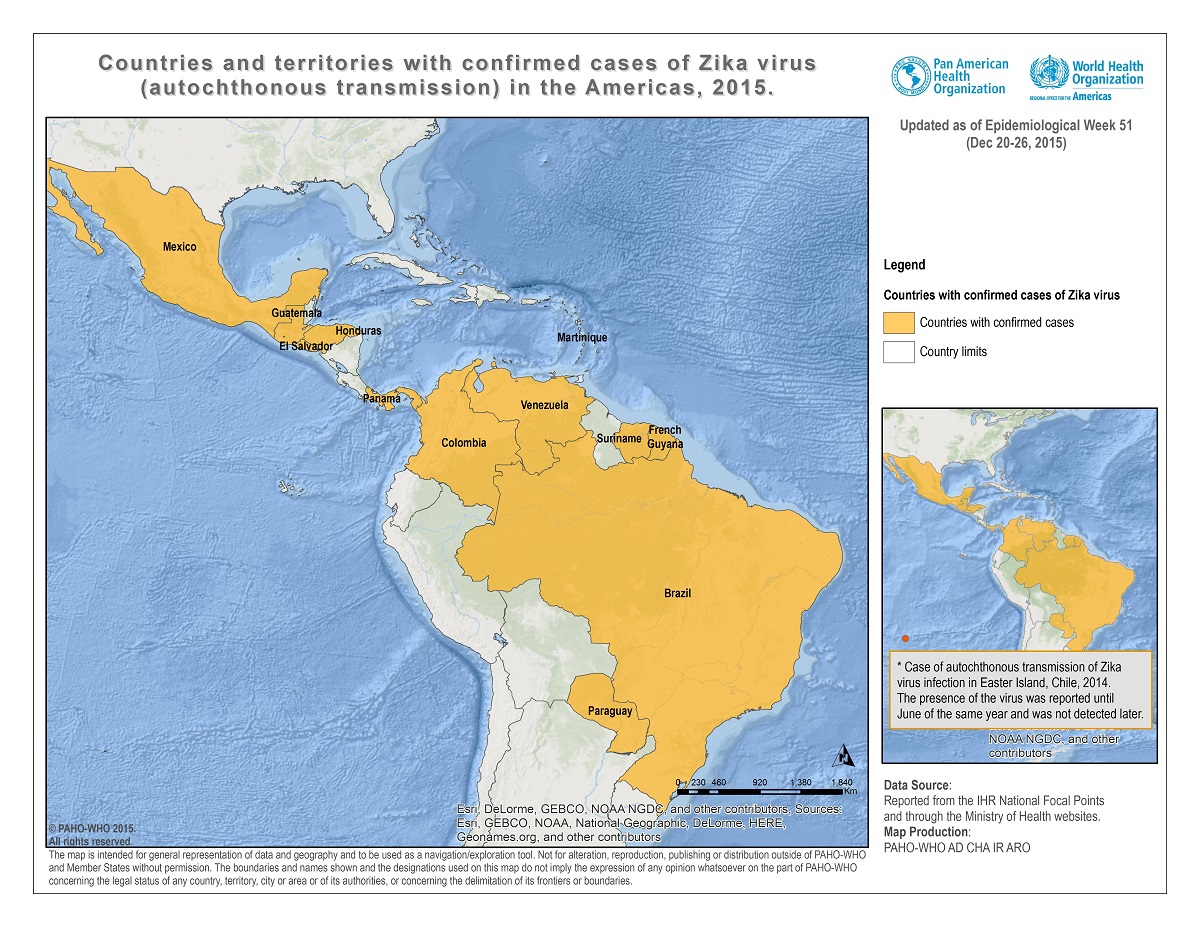
The CDC has issued travel advice for Zika Virus in South America earlier this month. Since its introduction to the Americas in 2014, Zika has now been reported in 14 South and Central American Countries, and is moving into the Caribbean, but Brazil is the most heavily impacted area to date.
The link between thousands of recently reported microcephalic births in Brazil and maternal infection with the Zika virus - while strongly suspected by Brazil's health authorities - has yet to be conclusively proven (see ECDC Rapid Risk Assessment – Zika & Microcephaly).
But given the severity of these birth defects, and the potential for rare potentailly serious neurological side effects from infection, an abudance of caution is warranted.
This posted today on the OSAC website.
Employee Health Safety; Disease Outbreak Western Hemisphere > Brazil; Western Hemisphere > Brazil > Brasilia 12/31/2015
The U.S. Embassy in Brasilia, Brazil informs U.S. citizens of a public health concern regarding the mosquito-transmitted Zika virus.
As dengue and chikungunya, the main transmitter of the Zika virus is the Aedes egypti, an urban mosquito that prefers to breed in and around homes. Large urban centers with surrounding poorer slums are ideal breeding grounds for Aedes egypti. Once infected mosquitoes become established in an area they are hard to contain.
The Zika virus is closely related to dengue. In 2007 the first known outbreak in humans occurred on the island of Yap in Micronesia and was followed by outbreaks in other Pacific Islands. Brazil reported its first case of Zika virus disease in May 2015.
Zika has often been called “dengue light.” Like dengue, only about 25 percent of those infected with Zika develop symptoms. These may include fever, headache, arthralgia (joint complaints), conjunctivitis (eye inflammation), and a maculopapular (red raised) rash that is generally not as severe as that caused by dengue or chikungunya. There are no hemorrhagic manifestations and no long term complications. People rarely become ill enough to require hospitalization. On rare occasions, there have been deaths associated with Zika infection.
Authorities are investigating a possible association between the Zika virus outbreak and increased numbers of babies born with microcephaly, a condition characterized by small head size and associated with cognitive impairment. As of the end of December, nine states in northeastern Brazil have reported 2,608 cases of microcephaly, a marked increase from previous years. As of the end of December, the state of Pernambuco has reported 150 affected babies - for 2015, compared with only 10 microcephalic babies reported in all of 2014. The Zika virus was found in the amniotic fluid of two affected babies. There is no indication that any pregnant woman needs to leave an area that has Zika infections at this time.
There is no vaccine or treatment for Zika, so prevention of mosquito bites is the only way to avoid infection. Pregnant women in particular should employ good personal protective measures to minimize the risk of Zika and other mosquito borne infections. These include use of CDC recommended topical repellants such as DEET or Picaridin, keeping arms and legs covered when outdoors and use of permethrin treated fabrics for clothing and tents.
Up to date information on the Zika virus, including the possible association between Zika virus and microcephaly, is available at http://www.cdc.gov/zika/.
Detailed information on protection against mosquito bites is available at http://wwwnc.cdc.gov/travel/yellowbook/2016/the-pre-travel-consultation/protection-against-mosquitoes-ticks-other-arthropods.
To obtain Centers for Disease Control and Prevention (CDC) travel notices, call the CDC at 1-800-CDC-INFO (1-800-232-4636) from within the United States, or 1-404-639-3534 from overseas, or visit the CDC website at http://www.cdc.gov/travel.
U.S. citizens should also consult the Department of State's Country Specific Information for Brazil which is located on the U.S. Department of State, Bureau of Consular Affairs website. Travelers may obtain up-to-date information on security conditions by calling 1-888-407-4747 toll-free in the United States and Canada, or on a regular toll line at 1-202-501-4444 from other countries. Stay up to date by bookmarking our Bureau of Consular Affairs website which contains current Travel Warnings and Travel Alerts.
Regularly monitor the State Department's website, where you can find current Travel Warnings, Travel Alerts, and the Worldwide Caution. Read the Country Specific Information for Brazil. For additional information, refer to "A Safe Trip Abroad" on the State Department's website.
We strongly recommend that U.S. citizens traveling to or residing in Brazil to enroll in the Department of State’sSmart Traveler Enrollment Program (STEP) at www.Travel.State.Gov. STEP enrollment gives you the latest security updates, and makes it easier for the U.S. embassy or nearest U.S. consulate to contact you in an emergency. If you don’t have Internet access, enroll directly with the nearest U.S. embassy or consulate.
.svg/275px-Jiangxi_in_China_(%2Ball_claims_hatched).svg.png)