Twenty-four years ago a study looked at the rate of heart attacks in the United States, and confirmed what every paramedic and ER doctor already knew; that Acute Myocardial Infarctions (AMIs) run as much 53% higher during the winter months than than during the summer.
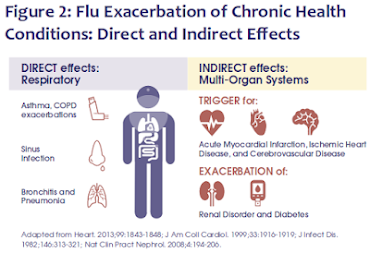
While many theories have been offered (holiday stress, cold weather, over-indulgence during the holidays, etc.), a growing number of studies have shown that Influenza - and other acute respiratory infections - can act as triggers for heart attacks and strokes.
A few (of many) featured in this blog include:
- In 2015, in UNSW: Flu Vaccine Provides Significant Protection Against Heart Attacks,we saw a study that found that if you are over 50 - getting the flu vaccine can cut your risk of a heart attack by up to 45%.
- In 2018, a study appearing the American Heart Association's journal Circulation, found a substantial reduction in deaths among heart failure patients who received a yearly flu shot (see AHA: Study Shows Flu Shots Reduce Deaths From Heart Failure).
- In January 2019, in Chest: Flu Vaccine Reduces Severe Outcomes Among Hospitalized Patients With COPD, researchers found a lower mortality rate, less critical illness, and a 38% reduction in influenza-related hospitalizations in vaccinated vs unvaccinated individuals.
- Also in 2019, in Flu Vaccine May Lower Stroke Risk in Elderly ICU Patients, we saw a study that found influenza vaccinated ICU survivors had a lower 1-year risk of stroke and a lower 1-year risk of death than unvaccinated survivors.
While the flu vaccine doesn't guarantee you'll avoid infection, most years it provides moderately good protection against circulating influenza viruses. And for those who are vaccinated - but still get the flu - they are less likely to have a severe bout.
ARTICLES| VOLUME 10, ISSUE 12, E1835-E1844, DECEMBER 01, 2022
Influenza vaccine to reduce adverse vascular events in patients with heart failure: a multinational randomised, double-blind, placebo-controlled trial
Prof Mark Loeb, MD Prof Ambuj Roy, MD Hisham Dokainish, MD Prof Antonio Dans, MD Prof Lia M Palileo-Villanueva, MD Prof Kamilu Karaye, MD et al.Open AccessPublished:December, 2022DOI:https://doi.org/10.1016/S2214-109X(22)00432-6
Summary
Background
Influenza increases the risk of cardiovascular events and deaths. We aimed to see whether influenza vaccination reduces death and vascular events in patients with heart failure.
Methods
We did a pragmatic, randomised, double-blind, placebo-controlled trial in 30 centres (mostly hospitals affliated with universities or a research institute) in ten countries in Asia, the Middle East, and Africa (7 in India, 4 in Philippines, 4 in Nigeria, 6 in China, 1 in Zambia, 2 in Mozambique, 3 in Saudi Arabia, 1 in Kenya, 1 in Uganda, and 1 in Zambia). Participants (aged ≥18 years; 52·1% female; not disaggregated by race or ethnicity) with heart failure (New York Heart Association class II, III, or IV) were randomly assigned (1:1) by a centralised web-based system with block randomisation stratified by site, to receive 0·5 ml intramuscularly once a year for up to 3 years of either inactivated standard dose influenza vaccine or placebo (saline). We excluded people who had received influenza vaccine in 2 of the previous 3 years, and those likely to require valve repair or replacement. Those who administered assigned treatments were not masked and had no further role in the study. Investigators, study coordinators, outcome adjudicators, and participants were masked to group assignment. The first of two co-primary outcomes was a first-event composite for cardiovascular death, non-fatal myocardial infarction, and non-fatal stroke, and the second was a recurrent-events composite for cardiovascular death, non-fatal myocardial infarction, non-fatal stroke, and hospitalisation for heart failure. Outcomes were assessed every 6 months in the intention-to-treat population. Secondary outcomes were all-cause death, cardiovascular death, non-fatal myocardial infarction, non-fatal stroke, all-cause hospitalisation, hospitalisation for heart failure, and pneumonia, both overall and during periods of peak influenza exposure. This study is registered with ClinicalTrials.gov, NCT02762851.
Findings
Between June 2, 2015, and Nov 21, 2021, we enrolled 5129 participants and randomly assigned (1:1) 2560 (50·0%) to influenza vaccine and 2569 (50·0%) to placebo. The first co-primary outcome occurred in 380 (14·8%) of 2560 participants in the vaccine group and 410 (16·0%) of 2569 participants in the placebo group (hazard ratio [HR] 0·93 [95% CI 0·81–1·07]; p=0·30). The second co-primary outcome occurred in 754 (29·5%) of 2560 participants in the vaccine group and 819 (31·9%) of 2569 participants in the placebo group; HR 0·92 [95% CI 0·84–1·02]; p=0·12). The secondary outcomes of all-cause hospitalisations (HR 0·84 [95% CI 0·74–0·97]; p=0·013) and pneumonia (HR 0·58 [0·42–0·80]; p=0·0006) were significantly reduced in the vaccine group compared with in the placebo group but there was no significant difference between groups for all-cause death, cardiovascular death, non-fatal myocardial infarction, non-fatal stroke, and hospitalisation for heart failure. In a prespecified analysis, in which events were limited to periods of peak influenza circulation, the first co-primary outcome, and the secondary outcomes of all-cause death, cardiovasular death, and pneumonia were significantly lower in the vaccinated group than in the placebo group, whereas the second co-primary outcome and the secondary outcomes of non-fatal myocardial infarction, non-fatal stroke, all-cause hospitalisation, and hospitalisation for heart failure were not significantly lower.
Interpretation
Although the prespecified co-primary outcomes during the entire period of observation were not statistically significant, the reduction during the peak influenza circulating period suggests that there is likely to be a clinical benefit of giving influenza vaccine, given the clear reduction in pneumonia, a moderate reduction in hospitalisations, and a reduction in cardiovascular events and deaths during periods of peak circulation of influenza. Taken in conjunction with previous trials and the observational studies, the collective data suggest benefit.
The press release from McMaster University in Ontario, Canada:
NEWS RELEASE 15-NOV-2022
Flu shots can protect patients with heart failure from death
by reducing cardiac complications as well as preventing influenza in people with with cardiovascular disease
MCMASTER UNIVERSITY
Hamilton, ON (Nov. 15, 2022) – Flu shots can save the lives of people with cardiovascular disease by reducing cardiac complications as well as preventing influenza.
An international study led by McMaster University researchers and published in The Lancet Global Health has found that influenza vaccines greatly reduce both pneumonia and cardiovascular complications in people with heart failure.
“If you have heart failure, you should get your flu shot because it can save your life – that is what we found in this study,” said the study’s principal investigator Mark Loeb.
Loeb is a McMaster professor of pathology and molecular medicine and a Hamilton infectious disease physician and microbiologist.
“It is underappreciated that influenza vaccine can save people from cardiovascular death,” he added.
The study showed that over the entire year the influenza vaccine reduced pneumonia by 40 per cent and hospitalization by 15 per cent in patients with heart failure. During influenza season in the fall and winter, the influenza vaccine reduced deaths by 20 per cent in these patients.
Data gathered during flu season also showed the vaccine helped protect against cardiovascular complications, such as heart attacks and strokes.
This collaborative clinical trial between McMaster and the Population Health Research Institute of McMaster and Hamilton Health Sciences, had investigators track more than 5,000 patients with heart failure in 10 countries across Africa, Asia and the Middle East where few people have regular influenza vaccination. They received either an influenza vaccine or a placebo annually between June 2015 and November 2021.
While the flu has long been associated with an increased risk of life-threatening cardiovascular events, Loeb said that people with heart failure are already vulnerable to poor health outcomes. Patients with the condition have a 50 per cent chance of dying within five years, while 20 per cent are hospitalized for cardiovascular complications every year.
reduced deaths
“Importantly, we looked at low and middle-income countries where 80 per cent of cardiovascular disease occurs and where flu vaccination rates are low.”
Salim Yusuf, executive director of PHRI and an author of the study said: “The flu shot should be part of the standard practise in people with heart failure given how simple, inexpensive and safe it is. Avoiding one sixth of deaths from heart disease and preventing hospitalizations makes it very cost effective and that can have an important public health and clinical impact.”
The study is the first clinical trial of the flu vaccine’s effectiveness in patients with heart failure.
External funding for the study came from the Joint Global Health Trials Scheme of the U.K. and by the Canadian Institutes of Health Research. The vaccines used for the study were provided by Sanofi Pasteur.
Despite an early, and aggressive, 2022-2023 flu season, uptake of flu vaccines around the country remain disappointingly low. From the CDC's Weekly Flu Vaccination Dashboard:
Coverage for the 2022-23 season as of October 15, 2022:
- Overall coverage at the end of September 2022 was 5.4 percentage points lower compared with the end of September 2021 (21.0% compared with 26.4%) and 17 percentage points lower than at the end of September 2020 (21.0% compared with 38.0%).
Despite its known limitations, getting the yearly flu vaccine – along with practicing good flu hygiene (washing hands, covering coughs, & staying home if sick) – remains your best strategy for avoiding the flu and staying healthy this winter.
And with our concurrent COVID pandemic, anything that can help keep you out of the hospital this fall and winter is worth considering.