#17,298
Not quite two weeks ago, in Bangladesh: Nipah Outbreak Update & ECDC Risk Assessment, we looked at early media reports of a Nipah virus outbreak in which Health Minister Zahid Malek, was quoted as saying:
'8 people have been infected with Nipah virus in our country this time. 5 of them have died. There are no new cases. 25-bed units have been opened in 2 hospitals for Nipah virus and 28 districts have been alerted.'
Carried by fruit bats, outbreaks often occur between December and May - which is date palm sap harvesting season - as infected bats often roost at night at the top of date palm trees, and collection containers can become contaminated with bat saliva and feces.
There are other routes of infection, as we saw in Malaysia in 1998 when the spread first from bat to pigs - and then from pigs to humans - eventually infecting at least 265 people, killing 105 (see Lessons from the Nipah virus outbreak in Malaysia).
Human-to-human transmission has also been reported, as in India in 2018 (see Nipah Transmission In Kerala Outbreak) where we saw apparently robust household and nosocomial transmission of the virus in Southern India, eventually infecting 19 people.
Since that initial report, we've seen the number of infections increase, as well as the number of deaths (see IEDCR Confirms 10 Nipah Cases & 7 Deaths). Overnight the WHO published their first update and risk assessment, which increases the case count to 11, and the number of deaths to 8.
First, some excerpts from this report, after which I'll return with a postscript.
Nipah virus infection - Bangladesh
17 February 2023
Situation at a glance
Nipah virus infection outbreaks are seasonal in Bangladesh, with cases usually occurring annually between December and May. Since the report of the first case in 2001, the number of yearly cases has ranged from zero to 67, though in the last five years, reported cases have been comparatively lower ranging from zero in 2016 to eight in 2019.
However, since 4 January 2023 and as of 13 February 2023, 11 cases (10 confirmed and one probable) including eight deaths (Case Fatality Rate (CFR) 73%) have been reported across two divisions in Bangladesh.
A multisectoral response has been implemented by the Ministry of Health and Family Welfare, Bangladesh, including strengthened surveillance activities, case management, infection prevention and control, and implementation of risk communication campaigns.
WHO assesses the risk as high at the national level, moderate at the regional level, and low at the global level.
(SNIP)
Epidemiology of Nipah virus infection
Nipah virus infection is an emerging bat-borne zoonotic disease transmitted to humans through infected animals or contaminated food. It can also be transmitted directly from person to person through close contact with an infected person. Fruit bats or flying foxes (Pteropus species) are the natural hosts for Nipah virus.
The incubation period is believed to range from 4 to 14 days. However, an incubation period up to 45 days has been reported. Laboratory diagnosis of a patient with a clinical history of Nipah virus infection can be made during the acute and convalescent phases of the disease by using a combination of tests. The main tests used are RT-PCR from bodily fluids and antibody detection via ELISA.
Nipah virus infection in humans causes a range of clinical presentations, from asymptomatic infection (subclinical) to acute respiratory infection and fatal encephalitis. Infected people initially develop symptoms including fever, headaches, myalgia (muscle pain), vomiting, and sore throat. This can be followed by dizziness, drowsiness, altered consciousness, and neurological signs that indicate acute encephalitis. Some people can also experience atypical pneumonia and severe respiratory problems, including acute respiratory distress. Encephalitis and seizures occur in severe cases, progressing to coma within 24 to 48 hours. Most people who survive acute encephalitis make a full recovery, but long-term neurologic conditions have been reported in survivors. Approximately 20% of patients are left with residual neurological consequences such as seizure disorder and personality changes. A small number of people who recover subsequently relapse or develop delayed onset encephalitis.
The overall global case fatality rate is estimated at 40% to 75% depending on local capabilities for epidemiological surveillance and clinical management. Although antivirals are in development, there are no licensed vaccines or therapeutics available for the prevention or treatment of Nipah virus infection.
(SNIP)
WHO risk assessment
The overall risk is assessed by WHO as high at the national level due to the following reasons:
- Although Nipah virus cases are reported in Bangladesh almost every year, 11 cases and eight deaths, have already been reported in 2023, which is unusual compared to the past seven years.
- The case fatality rate from Nipah virus infection is high (73%). Initial signs and symptoms of Nipah virus infection are non-specific, and the diagnosis is often not suspected at the time of presentation. This can hinder accurate diagnosis and creates challenges in outbreak detection, effective and timely infection control measures, and outbreak response activities.
- There are currently no specific drugs or vaccines available for Nipah virus infection although WHO has identified Nipah as a priority disease for the WHO Research and Development Blueprint. Intensive supportive care is recommended to treat severe respiratory and neurologic complications.
- Currently, the level of awareness among the general population is still low, despite ongoing efforts for risk communication and community engagement.
- There has already been one case of suspected human-to-human transmission during the current outbreak and secondary cases have previously been reported in Bangladesh.
- Fruit bats or flying foxes (Pteropus species.), the natural reservoir of Nipah virus, is present in Bangladesh and the genetic diversity of Nipah virus isolated from affected persons in Bangladesh suggest substantial diversity of the virus in the wildlife reservoir and repeated spill over of the virus from its reservoir to the human population.
The risk at the regional level is moderate as Rajshahi district borders India. Although there have not been any instances of cross-border transmission by humans previously, this risk remains given the shared ecological corridor for the virus’s natural host (fruit bats or flying foxes) and occurrence among domestic animals and humans previously in both countries. India also has experienced previous outbreaks of Nipah virus infection.
The risk assessed at the global level is low considering the absence of natural hosts in many countries and the fact that there have been no previous cases outside Bangladesh, India, Malaysia, and Singapore.
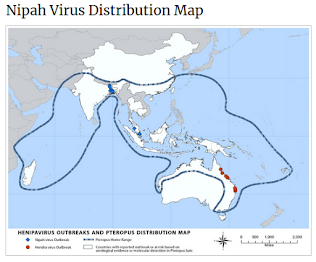
Given the limits of testing and surveillance, it is likely that some number of cases in Bangladesh, and in neighboring countries, go unidentified each year, as the geographic range of the fruit bat that carries the virus is quite large (see map at top of blog).
Outbreaks in humans since the virus was first identified in the late 1990s have tended to be sporadic, and small - although the largest, in Malaysia (1998-1999), saw 265 infected and 105 deaths.
In the 2013 paper The pandemic potential of Nipah virus by Stephen P. Luby, the author wrote (bolding mine):
Characteristics of Nipah virus that increase its risk of becoming a global pandemic include: humans are already susceptible; many strains are capable of limited person-to-person transmission; as an RNA virus, it has an exceptionally high rate of mutation: and that if a human-adapted strain were to infect communities in South Asia, high population densities and global interconnectedness would rapidly spread the infection.
And after the 2018 outbreak in Kerala, India, concerns over larger, urban outbreaks of the virus have increased (see Enhancing preparation for large Nipah outbreaks beyond Bangladesh: Preventing a tragedy like Ebola in West Africa by Halsie Donaldson, Daniel Lucey).
Whether Nipah has - or will ever accrue - the `right stuff' to pose a genuine pandemic threat is unknowable.
But in 2019 the WHO published their List Of Blueprint Priority Diseases, detailing 8 disease threats in need of urgent accelerated research and development. And Nipah, and its Australian cousin Hendra, were among them.
For more on Nipah, Hendra, and other henipaviruses you may wish to revisit: