#17,571

Officially the WHO has received just over 2,600 case reports, of which 36% (n=936) proved fatal.
Even when countries are aggressively looking for cases, detecting MERS-CoV can be difficult, and official case counts are assumed to be under counts (see EID Journal: Estimation of Severe MERS Cases in the Middle East, 2012–2016. Some past blogs on these challenges include:
EID Journal: Sensitivity and Specificity Of MERS-CoV Antibody Testing
AJIC: Intermittent Positive Testing For MERS-CoV
JIDC: Atypical Presentation Of MERS-CoV In A Lebanese Patient
Yesterday the World Health Organization published the following update after the notification by the UAE of a MERS infection in an apparently healthy 28-year old male, who was not a healthcare worker (a known risk factor), and who had no known contact with camels or camel products.
The patient was admitted to the hospital on June 8th with gastrointestinal symptoms (including diarrhea), referred to the ICU at `a specialized government tertiary hospital' on June 13th and placed on a ventilator, but testing for MERS wasn't done until June 21st, and results weren't known until the 23rd; 15 days after first entering the hospital.
Since failure to make a MERS diagnosis not only endangers the patient, it risks sparking a major nosocomial outbreak, in response the Abu Dhabi Public Health Centre (ADPHC) has reportedly `. . . updated the case definition for MERS-CoV, strengthened surveillance activities to identify possible cases, conducted several workshops and issued circulars for MERS-CoV.'
First some excerpts from the WHO update, then I'll return with a postscript. Follow the link to read it in its entirety.
Middle East Respiratory Syndrome - United Arab Emirates
24 July 2023
Situation at glance:
On 10 July 2023, the United Arab Emirates (UAE), notified WHO of a case of Middle East Respiratory Syndrome Coronavirus (MERS-CoV) in a 28-year-old male from Al Ain city in Abu Dhabi. The case had no history of direct or indirect contact with dromedaries, goats, or sheep.
The patient was admitted to the hospital on 8 June. A nasopharyngeal swab was collected on 21 June and tested positive for MERS-CoV by polymerase chain reaction (PCR) on 23 June 2023. All 108 identified contacts were monitored for 14 days from the last date of exposure to the MERS-CoV patient. No secondary cases have been detected to date.
Since July 2013, when the UAE reported the first case of MERS-CoV, 94 confirmed cases (including this new case) and 12 deaths have been reported. Globally, the total number of confirmed MERS-CoV cases reported to WHO since 2012 is 2605, including 936 associated deaths.
WHO continues to monitor the epidemiological situation and conducts risk assessments based on the latest available information. WHO expects that additional cases of MERS-CoV infection will be reported from the Middle East and/or other countries where MERS-CoV is circulating in dromedaries.
WHO re-emphasizes the importance of strong surveillance by all Member States for acute respiratory infections, including MERS-CoV, and to carefully review any unusual patterns.
Description of the case:
On 10 July 2023, the International Health Regulations National Focal Point (IHR NFP) of the United Arab Emirates (UAE) notified WHO of a confirmed case of MERS-CoV in Abu Dhabi. The patient is a 28-year-old male, non- Emirati national living in Al Ain city, a non-healthcare worker. The case visited a private medical center multiple times between 3 and 7 June 2023, complaining of vomiting, right flank pain, and dysuria (pain when passing urine). On 8 June, the case presented to a government hospital with vomiting, and gastrointestinal symptoms including diarrhea, and was given an initial diagnosis of acute pancreatitis, acute kidney injury, and sepsis.
On 13 June, he was in critical condition and referred to an intensive care unit (ICU) at a specialized government tertiary hospital where he was put on mechanical ventilation. He deteriorated and a nasopharyngeal swab was collected on 21 June and tested positive for MERS-CoV by PCR on 23 June 2023.
The case has no known co-morbidities, no history of contact with MERS-CoV human cases, and no recent travel outside the UAE. The patient has no known history of direct contact with animals including dromedary camels, nor consumption of their raw products.
All 108 contacts that were identified have been monitored for 14 days from the last date of exposure to the MERS-CoV patient, no secondary case was identified. The case has no family members or household contacts identified in the UAE.
Prior to this notification, the last MERS-CoV infection reported from the UAE was in November 2021. The first laboratory-confirmed case of MERS-CoV in UAE was in July 2013. Since then, the UAE has reported 94 cases of MERS-CoV (including this current case) and 12 associated deaths (Case Fatality Ratio (CFR): 13%).(SNIP)
WHO risk assessment
Middle East Respiratory Syndrome (MERS) is a viral respiratory infection of humans and dromedary camels which is caused by a coronavirus called the Middle East Respiratory Syndrome Coronavirus (MERS-CoV). Infection with MERS-CoV can cause severe disease in humans resulting in high mortality. Approximately 35% of patients with MERS-CoV have died, but this may be an overestimate of the true mortality rate, as mild cases of MERS-CoV may be missed by existing surveillance systems. Until more is known about the disease, the case fatality rates are counted only amongst the laboratory-confirmed cases reported to WHO.
Humans are infected with MERS-CoV from direct or indirect contact with dromedaries, a host and zoonotic source of MERS-CoV infection. MERS-CoV has demonstrated the ability to be transmitted between humans. So far, the observed non-sustained human-to-human transmission has occurred among close contacts and in healthcare settings. Outside of the healthcare setting, there has been limited human-to-human transmission.
Cases of MERS-CoV infection are rare in the UAE. Since July 2013, a total of 94 MERS-CoV cases, including this current case, resulting in 12 deaths (CFR 13%) have been reported to WHO from the UAE.
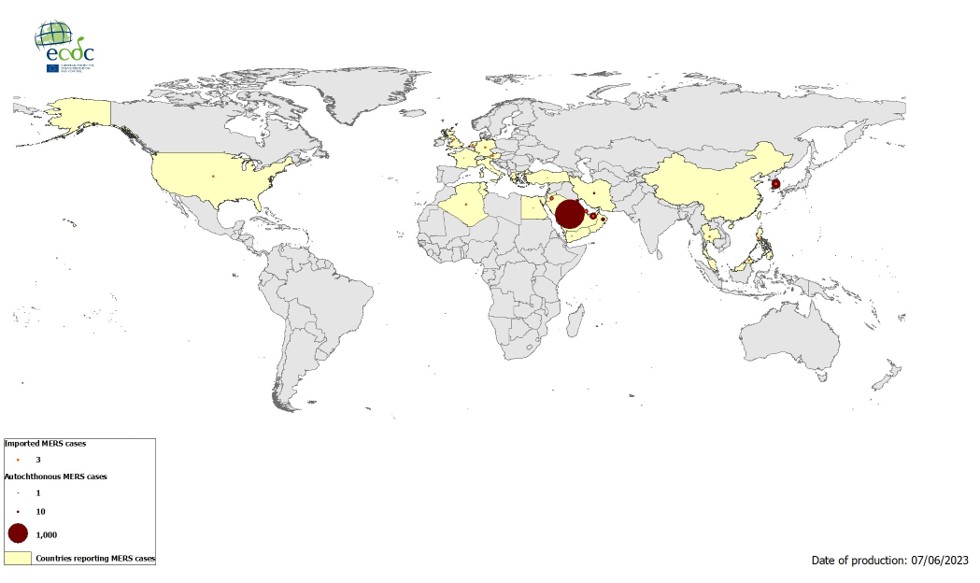
Globally, the total number of laboratory-confirmed MERS-CoV cases reported to WHO since 2012 is 2605, including 936 associated deaths as of July 2023. The majority of the reported cases have occurred in countries in the Arabian Peninsula. Outside of this region, there has been one large outbreak in the Republic of Korea, in May 2015, during which 186 laboratory-confirmed cases (185 in the Republic of Korea and one in China) and 38 deaths were reported. The global number reflects the total number of laboratory-confirmed cases and deaths reported to WHO under IHR (2005) to date.
The notification of this case does not change the overall risk assessment. WHO expects that additional cases of MERS-CoV infection will be reported from the Middle East and/or other countries where MERS-CoV is circulating in dromedaries, and that cases will continue to be exported to other countries by individuals who were exposed to the virus through contact with dromedaries or their products (for example, consumption of camel’s raw milk), or in a healthcare setting.
WHO continues to monitor the epidemiological situation and conducts risk assessments based on the latest available information.
Prior to the emergence of SARS-CoV-2 in late 2019, MERS-CoV was the coronavirus with the most pandemic potential (see 2017's A Pandemic Risk Assessment Of MERS-CoV In Saudi Arabia), and while COVID beat it to the punch, it remains very much a threat.
Last April, in IJID: MERS-CoV – A Ten-year (2012-2022) Global Analysis of Human and Camel infections, we looked at an excellent review, and analysis, of the the spread and evolution of MERS-CoV in camels and humans over the past decade. Among the highlights:
- MERS-CoV remains on the WHO priority pathogens list
- WHO reports 2,184 out of a total of 2591 human MERS cases are from Saudi Arabia
- Three MERS-CoV Clades were identified: Clade B(n=462), clade A(n=10), clade C(n=5)
- New MERS-CoV variants and co-infections continue to circulate in camels
- Proactive virus surveillance and genomic analyses in camels and humans is required
There are some researchers who worry that MERS-COV and SARS-CoV-2 could some day recombine into a hybrid (see Nature: CoV Recombination Potential & The Need For the Development of Pan-CoV Vaccines) resulting in either a `SARS-CoV-3' or `MERS-CoV-2' virus.
How likely that is to happen is a subject of considerable debate, but it appears to be at least theoretically possible.
Human-to-human transmission of MERS-CoV in healthcare settings has been associated with delays in recognizing the early symptoms of MERS-CoV infection, slow triage of suspected cases and delays in implementing infection, prevention and control (IPC) measures.
IPC measures are therefore critical to prevent the possible spread of MERS-CoV between people in health-care facilities. Health -care facilities should ensure environmental and engineering controls are in place including adequate ventilation, spatial separation of at least one meter between patients and others, including health and care workers and adequate environmental cleaning.
Health care workers should consistently apply standard precautions to all patients at every interaction in healthcare settings. Droplet precautions, including eye protection, should be applied in addition to standard precautions when providing care to patients with symptoms of acute respiratory infection; contact precautions should be added when caring for probable or confirmed cases of MERS-CoV infection; airborne precautions should be applied when performing aerosol-generating procedures or in settings where aerosol-generating procedures are conducted.
Early identification, case management and isolation of cases, quarantine of contacts, appropriate infection prevention and control measures in health care settings, and public health awareness can prevent human-to-human transmission of MERS-CoV.V
Variations of this advice have been repeated often over the past 10 years. Bu there is obviously still a lot of room for improvement.