#17,650
Not quite two months ago, in Italian MOH Statement: H5N1 Seroconversion In Dogs & Cats On Affected Poultry Farm In Brescia, we looked at the initial reports of yet another spillover of HPAI H5 into companion animals (see Media Reports Of Unusual Cat Deaths In Poland).
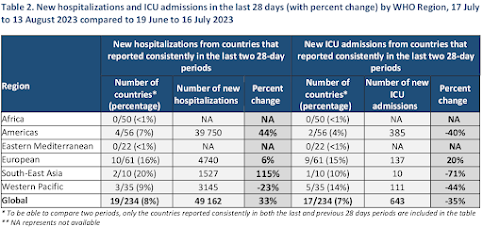
In early July the Italian website https://sivemp.it/ (Sindacato Italiano Veterinari Medicina Pubblica) carried a brief news story (link), which described the virus (isolated from the poultry) as HPAI H5N1 clade 2.3.4.4b of a genotype (BB) recently found in northern Italian gulls, and that it carried a rarely found mammalian adaption (T271A in the PB2 protein) that may increase its zoonotic potential.Unlike in Poland, these dogs and cats in Italy remained asymptomatic, and were only discovered due to aggressive testing of humans and other mammals on the affected farms (see chart above).
The puzzle being that this mutation - which has been found in a small percentage of mammals infected with the H5 clade 2.3.4.4b virus - has not been previously seen in infected avian species in Europe. This raises the possibility of transmission from mammals back to poultry.
Today the Journal Eurosurveillance has a follow up report, which includes a second round of serological testing of both humans and dogs. While no humans tested positive, the antibody titres in the dogs continued to show strong signs of past infection.
Due to its length, I've only reproduced the abstract, and the discussion/conclusion below. Follow the link to read the paper in its entirety.
Asymptomatic infection with clade 2.3.4.4b highly pathogenic avian influenza A(H5N1) in carnivore pets, Italy, April 2023
Ana Moreno1 , Francesco Bonfante2 , Alessio Bortolami2 , Irene Cassaniti3,4 , Anna Caruana8 , Vincenzo Cottini7 , Danilo Cereda5 , Marco Farioli5 , Alice Fusaro2 , Antonio Lavazza1 , Pierdavide Lecchini6 , Davide Lelli1 , Andrea Maroni Ponti6 , Claudia Nassuato7 , Ambra Pastori2 , Francesca Rovida3,4 , Luigi Ruocco6 , Marco Sordilli6 , Fausto Baldanti3,4,* , Calogero Terregino2,*
Since autumn 2021, highly pathogenic avian influenza A (HPAI) H5N1 clade 2.3.4.4b viruses have been detected in several continents [1] with a several spill-over events in mammals, which have raised concern about the ability of these viruses to infect and adapt to humans. The polymerase activity of avian influenza viruses (AIVs) is a known determinant of viral fitness. However, it is still unclear why the polymerase activity of viruses of avian origin is limited in mammalian cells. The adaptation of avian viruses to mammals, through natural selection processes leading to adaptive mutations in polymerase proteins, is an essential factor in increasing its replicative capacity in mammals [2,3].Here we report a case of influenza A(H5N1) infection in a domestic cat and five dogs living on a rural backyard poultry farm where an HPAI H5N1 outbreak was notified; the infection in poultry was caused by an HPAI H5N1 virus strain belonging to the BB genotype that was characterised by the presence of a PB2 mutation related to mammalian adaptation.
(SNIP)
Discussion
Here we report the serological evidence of HPAI H5N1 virus infection in five dogs and one cat on a rural farm in Italy. The virus identified in hens on the same farm, potentially responsible for the transmission of the virus to pet carnivores, belonged to the BB genotype, which emerged in Europe in May 2022 from reassortment events with the gull-adapted H13 subtype viruses, from which PA, NP and NS genes were acquired. In Italy, genotype BB was first identified in January 2023 and has spread widely in black-headed gulls in northern Italy, causing mass mortality events around Lake Garda in the same geographical area when the affected farm is placed [9]. This genotype was also responsible for seven outbreaks on commercial farms in the Veneto and Emilia Romagna regions [9]. Hence, its detection in this backyard farm in the Lombardy region was not unexpected, given its wide distribution among wild birds in the area surrounding the farm.
It was surprising to observe that the virus characterised in this study, detected in hens, differed from all other HPAI A(H5N1) clade 2.3.4.4b viruses circulating in poultry and in birds by a mutation in the PB2 protein, T271A, which is a marker of virus adaptation to mammalian species; it has previously been shown to be associated with increased polymerase activity in mammalian cells [2,10] and is present in the 2009 pandemic A(H1N1) virus [2]. It should be noted that this mutation has never been observed in H5Nx viruses of clade 2.3.4.4b collected from birds in Europe since 2020. In contrast, it has been detected in ca 7% of clade 2.3.4.4b viruses identified in mammals in Europe, including the virus responsible for the outbreak on a mink farm in Spain [15]. This molecular finding suggests that virus spread from mammals to birds cannot be excluded.
The recent cases of influenza A(H5N1) virus infections in domestic cats in France [16] and Poland [17] and in farmed fur animals across Finland [18] were initially detected because of their overt clinical manifestations characterised by severe respiratory distress and neurological signs; similar presentations are commonly associated with H5N1 cases in wild mammals [9].
In contrast, the affected pets in this report were completely asymptomatic, raising concerns over the possibility of subclinical infections with zoonotic viruses in animals in close contact with humans. The presence of antibody titres against HPAI H5 between 1:40 and 1:320 in the MN test suggests true infection rather than just exposure to the antigen. These results are in line with the recently published study by Chestakova et al. on a high number of HPAI H5 virus infections and antibodies in wild carnivores in the Netherlands during 2020–2022 [19]. In that study, antibody titres against HPAI H5 from 1:20 to 1:160 by HI test were detected and were considered indicative of natural infection even in the absence of clinical symptoms.
In addition, experimental challenge of Beagles with an H5N8 virus of clade 2.3.4.4b by nasal route presented a pathogenetic and clinical picture compatible with that observed in our case series, as the dogs showed few or no signs of infection with low nasal viral shedding, seroconversion with low HI titres, and transmission of infection to a sentinel contact [20].
The infection and transmission routes, as well as the pathogenicity of influenza A(H5N1) viruses in farmed and pet carnivores are still poorly understood. To improve our surveillance strategy and preparedness, further serological surveys and experimental research are needed to fully understand the ecology of H5N1 viruses in these animals.
Following the evolution of the epidemiological situation for HPAI and in light of the increasing signs of the circulating viruses’ adaptation to mammals, the Italian Ministry of Health has prepared, in the event of an outbreak of HPAI, specific surveillance plans for exposed people (Ministerial circular 0056437–08/12/2021-DGPRE-DGPRE-P) [21] and domestic carnivores (Device 0009342–04/04/2023 - DGSAF-MDS-P) [22] through syndromic, virological and serological surveillance.
Conclusions
This study highlights the importance of genetic surveillance to promptly detect viruses with increased zoonotic potential. Complete genomic sequencing of viruses is essential to identify the presence of gene mutations correlated with an adaptation of avian viruses to mammals.
As we've discussed previously, there are now dozens of genotypes of HPAI H5 clade 2.3.4.4b viruses circulating around the world, and many genetic variations may exist within each genotype.
It is not totally unexpected that dogs and cats infected with one genotype might experience severe illness or death, while those infected with another might remain asymptomatic.
And that's the rub. We aren't dealing with a single, monolithic, HPAI H5N1 virus. We are dealing with literally scores of similar avian viruses, on multiple continents, all pursuing their own evolutionary path.
Those viruses that remain in wild birds or poultry are expected to evolve differently than those that spill over into marine mammals, mink, or peridomestic animals.
The fact that some mammals - particularly companion animals - may be able to carry (and potentially spread) the virus without showing overt signs of illness, means that investigators will have to rely on more than cursory inspections when it comes to ruling out mammalian infections.