#17,675
Although influenza is frequently said to be `unpredictable', about 10 years ago the CDC began to investigate ways to anticipate its near-term moves (see CDC Competition Encourages Use of Social Media to Predict Flu), and since then the CDC's Influenza Division has collaborated with external researchers on flu forecasting.
Over time, and particularly since the start of the COVID pandemic, respiratory disease forecasting has evolved, with the Center for Forecasting and Outbreak Analytics (CFA) established in 2021, and officially launched in the spring of 2022.
Of course, there are always a lot of unknowns, and forecasting - while it is improving - remains in its infancy. Surprises are always possible. The CDC describes the difficulties:
Influenza (flu) places a significant disease burden on the U.S. population, but the magnitude and timing of flu activity varies from season to season, making the annual impact of flu uncertain at the beginning of each season. Flu forecasting can help decrease that uncertainty by predicting in advance when and where increases in flu activity will occur. Unlike CDC’s traditional influenza surveillance systems, which measure flu activity while it is occurring, flu forecasting offers the possibility of looking into the future and better planning ahead for changes, such as increases in flu-related hospitalizations.
(SNIP)
How can flu forecasts be used?
Flu forecasts can be used to prepare for changes in flu activity, such as increases in hospitalizations. When forecasts accurately predict flu activity, more effective planning of public health responses to seasonal flu epidemics and future flu pandemics is possible. Flu forecasts can inform messaging to health care providers regarding:
- antiviral treatment allocation,
- preparation for an influx of flu-related hospitalizations,
- informing the distribution and placement of health care staff, hospital beds and treatment resources.
Flu forecasts can also be used to help guide personal and community mitigation strategies. These can include non-pharmaceutical interventions, such as reducing contact during times of forecasted high flu activity, as well as conveying the importance of flu vaccination prior to forecasted increases in flu activity.
Yesterday, the CDC's CFA and NCIRD released a preliminary respiratory disease season `outlook' that presents a range of potential scenarios for this fall and winter. Basically, they anticipate a similar number of hospitalizations to what we saw last winter.
There are - as they point out - a lot of unknowns, including the future impact of BA.2.86.
As a result, they currently only have low-to-moderate confidence in this early assessment. I'll have a brief postscript after the break.
Respiratory Disease Season Outlook
Outlook
CDC expects the upcoming fall and winter respiratory disease season will likely have a similar number of total hospitalizations compared to last year. As with last year, the number of hospitalizations is expected to be higher than that experienced prior to the COVID-19 pandemic, when severe disease was caused primarily by the influenza virus and the respiratory syncytial virus (RSV).
However, it remains possible that hospitalizations this season may be higher than last year, with more widespread illness and healthcare system strain. This increase could result from the emergence of a new COVID-19 variant with an increased ability to evade the body’s prior immunity, or from a severe influenza season combined with COVID-19 and RSV waves that are similar to last year, or, as we saw last year, an increase in RSV infections. A key factor is the timing of the peak number of hospitalizations associated with each disease and whether those peaks coincide.
This outlook is based on expert judgment, historical data, and scenario modeling for COVID-19. We have low to moderate confidence in this assessment because of uncertainties in anticipating the timing of when diseases will peak and levels of disease.
Vaccination remains the best way to protect yourself and your loved ones against serious outcomes of these diseases. Vaccination is especially important for people who are at higher risk of developing serious complications.
CDC is offering this outlook to provide decision-makers information to assist with public health preparedness planning, including potential surges in hospital demand.
What is the rationale for this outlook for each disease?
Infectious disease experts and scenario models provide evidence that this season is likely to bring a moderate COVID-19 wave, causing around as many hospitalizations at the peak as occurred at last winter’s peak.
- There is widespread, population-level protective immunity to COVID-19 from prior infections and/or vaccinations, making it unlikely that COVID-19 will cause very large waves of severe disease or hospitalization, according to modeling by the COVID-19 Scenario Modeling Hub.
Experts anticipate that the influenza season will fall in the typical range of severity. However, even typical seasons vary widely in the number of illnesses, hospitalizations, and deaths.
- COVID-19 could peak earlier than last season, however, because of limited summer activity compared to past years.
Experts anticipate that RSV is likely to return to normal season patterns following a severe season last year.
- Experts do not believe that the COVID-19 pandemic—and associated interventions and behavior changes—will continue to have a major impact on influenza transmission, following reduced influenza activity in 2020-2021 and an early peak for the 2022-2023 season.
- Last year’s season likely elevated population immunity to typical levels, which had previously been lower because of reduced RSV circulation early in the COVID-19 pandemic.
- There are also new RSV prevention tools available, which could potentially decrease hospital burden. These include vaccines for those aged 60 years and older and an immunization for infants.
What are the key uncertainties?
High immunization uptake could reduce the number of hospitalizations substantially. i,ii,iii,iv It is difficult to predict the size and timing of peak activity for each disease, as well as how the timing might overlap. These factors will affect the level of strain on the healthcare system. There is also considerable uncertainty about the level of vaccine uptake, particularly for the RSV vaccine for older adults and RSV immunization for infants that are new this season.
The COVID-19 pandemic changed patterns for influenza and RSV circulation, and there could be lingering effects on population immunity or behavior that continue to affect influenza or RSV levels this season.
Other disease-specific uncertainties include the following:
- The virus that causes COVID-19 is constantly changing, and a new variant could emerge which is less effectively mitigated by immunity from past infections or from existing vaccines and treatments. COVID-19 has not yet occurred as a regular seasonal disease, so we do not yet fully understand how the timing and magnitude of waves will vary.
- We do not yet know which influenza viruses will predominate, which can affect the number of severe illnesses and hospitalizations. We also do not yet know how effective vaccines will be against the predominant viruses.
- Particularly for RSV, we have less precise estimates for the burden of illnesses and hospitalizations data on past seasons to inform expectations for this fall/winter.
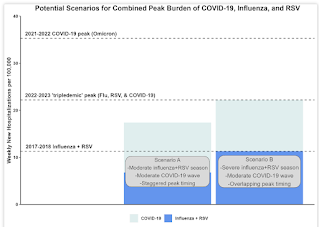
What are some potential scenarios for the peak hospital demand during the upcoming season?
CDC developed two hypothetical scenarios for the peak hospital burden of COVID-19, influenza, and RSV. These scenarios illustrate how the additional burden from COVID-19 during a moderate season for the three respiratory diseases may generate more hospital demand – potentially resulting in hospital strain – than a severe influenza and RSV season prior to the emergence of COVID-19 (Figure 1).
The graph above shows that a moderate influenza and RSV season with a moderate COVID-19 wave (the combined bar on the left) could generate more hospital strain than a severe, pre-COVID-19 influenza and RSV season (the dark blue bar on the right). While we cannot predict the precise timing and impact of these three pathogens each season, these are two plausible scenarios.

- In scenario A, we combine a moderate past season peak for influenza and RSV equal to 2019-20 with a moderate COVID-19 wave equal to winter 2022-23. We also shift the timing of the COVID-19 wave so that the peak occurs three weeks prior to the peak of influenza + RSV hospitalizations. In this scenario, the peak hospitalization rate is roughly 20% lower than the 2022-2023 peak. The peak is higher than the level for a severe season of influenza and RSV combined, as illustrated by Scenario B.
- In scenario B, we combine a severe past season peak for influenza and RSV equal to 2017-18 with a moderate COVID-19 wave equal to winter 2022-23. We also shift the timing of the COVID-19 wave so that its peak occurs in the same week as influenza + RSV peak hospitalizations. In this scenario, the peak hospitalization rate is similar to that of the 2022-2023 season and slightly higher than the peak hospitalization rate for COVID-19 alone in the 2020-2021 season.
How does the emergence of new COVID-19 variants such as BA.2.86 affect this outlook?
At this time, we do not know enough about BA.2.86 to assess its potential impact on the upcoming disease season, though the scenarios outlined here likely account for the emergence of a wide range of variants.
CDC is continually monitoring for new variants and studying their potential impact on public health. Scientists are evaluating the effectiveness of the updated COVID-19 vaccine.
CDC’s current assessment is that this updated vaccine will be effective at reducing severe disease and hospitalization. At this point, there is no evidence that this variant is causing more severe illness. That assessment may change as additional scientific data are collected.
We are monitoring carefully and will update this outlook as we learn more.
How will CDC monitor respiratory illnesses this season?
CDC has a robust system of domestic and global monitoring and early warning systems, which include tracking data on hospitalizations, emergency department visits, laboratory tests, genomic sequencing, and wastewater testing.
CDC is also working to improve real-time analysis and forecasting for these diseases. CDC produces regular influenza forecasts throughout the season. For COVID-19, we are producing regular forecasts and working to improve these predictions through integrating past data on COVID-19 activity to understand seasonal variation in epidemic timing and magnitude.
CDC will update this outlook as we learn more about respiratory virus activity this season.
This outlook was prepared by CDC’s Center for Forecasting and Outbreak Analytics (CFA) and National Center for Immunization and Respiratory Diseases (NCIRD).
Since I'm pushing 70, I remember the day weather forecasting changed forever; April 1st 1960. The day that TIROS I - the world's first weather satellite - was launched into Earth orbit from Cape Canaveral, Florida.
TIROS 1 could take and transmit about 1 picture an hour, but only during daylight hours (infrared capability was added to later `birds'). And while the pictures were grainy, and the resolution laughable by today's standards, for the first time we could watch from space and see how and where hurricanes formed.

It meant we were no longer solely dependent on ship's reports and Hurricane Hunter aircraft to know if disaster was creeping just beyond the horizon. It meant coastal residents could count on more than 12 hours warning to prepare for a storm.
Sixty years later, hurricanes can still sometimes fool us (e.g. Ian, Dorian, etc.), but we are far more confident in their forecast paths than we were even a decade or two ago.
As far as this outlook is concerned, a lot will depend upon the uptake of influenza, COVID, and RSV vaccines in the months ahead.