 |
| Number of severe influenza cases by Age Groups - Flu Express Week 9 |
#13,183
As the Flu Express chart above indicates, Hong Kong has endured two severe influenza outbreaks in the last 8 months, with only about a 4 month respite between their summer and winter epidemics. Last summer the culprit was Influenza A/H3N2 while this winter they have been battered (along with Mainland China) with Influenza B.
While Hong Kong is known for having a biphasic or `double peaked’ flu season, it is rare to see two back-to-back severe outbreaks in a single year (see Seasonality of Influenza A(H3N2) Virus: A Hong Kong Perspective (1997–2006).Two long months after this winter's epidemic was declared, there are hopeful signs that influenza has peaked in Hong Kong, and is starting to decline. Consultations for ILI are down over last week, and while still high, hospital occupancy rates are lower as well.
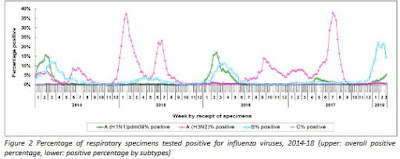
With Influenza B rates starting to decline (see chart below), we are seeing signs Influenza A/H1N1 detections are starting to rise. We've seen similar trends reported from Mainland China (see Shenzhen Port Authorities Increase Health Inspections As Influenza Cases Rise) and so this will be something to keep an eye on in the weeks ahead.
It is likely that the high incidence of Influenza A last summer opened the door for influenza B to dominate this winter. That temporary community immunity may be starting to wane.
One of the most dramatic indicators of how rough this winter's flu season has been are the number of institutional outbreaks (schools, residential care facilities) reported. Despite a 2-week extended school closure, they far exceed anything reported in recent years.

As the following chart illustrates, Hong Kong (pop 7 million) has seen a large number of severe and/or fatal cases this winter, with the elderly (65+) and Baby Boomers (50-64) the hardest hit groups.

The following two charts compare the number of ICU admissions and deaths from this winter's flu season to the last few year's severe flu outbreaks.

They indicate that the number of ICU admissions are higher than during the severe 2014-15 H3N2 outbreak, but the number of deaths (after 8 weeks) are roughly the same. Compared to last summer's extended influenza A epidemic (blue line), this winter's outbreaks has gotten off to a very rapid start.
A few more selected excerpts from today's (Week 9) Hong Kong Flu Express:
FLU EXPRESS
Flu Express is a weekly report produced by the Respiratory Disease Office of the Centre for Health Protection. It monitors and summarizes the latest local and global influenza activities.
Local Situation of Influenza Activity (as of Mar 7, 2018)
Reporting period: Feb 25 – Mar 3, 2018 (Week 9)
(SNIP)
- The latest surveillance data showed that the local influenza activity has started to decrease but is still at a high level. It is foreseen that the local influenza activity will remain elevated for some time. Currently the predominating virus is influenza B.
- Influenza can cause serious illnesses in high-risk individuals and even healthy persons. Given that seasonal influenza vaccines are safe and effective, all persons aged 6 months or above except those with known contraindications are recommended to receive influenza vaccine to protect themselves against seasonal influenza and its complications, as well as related hospitalisations and deaths.
- Apart from adopting personal, hand and environmental hygiene practices against respiratory illnesses, those members of the public who have not received influenza vaccine are urged to get vaccinated as soon as possible for personal protection.
Global Situation of Influenza Activity
- In Mainland China (week ending Feb 18, 2018), both southern and northern provinces were still in winter influenza season. Although the proportion of ILI cases in emergency and outpatient departments increased as a result of decreased number of patients attending hospitals during the Lunar New Year holiday, the proportion of influenza detections was on a decreasing trend. Currently the influenza activity in southern provinces was higher than that in northern provinces. The proportion of influenza A detection was higher than that of influenza B. Influenza A(H1N1) and influenza B Yamagata viruses are predominating while levels of influenza A(H3N2) and influenza B Victoria viruses remained low. In southern provinces, the proportion of ILI cases in emergency and outpatient departments reported by sentinel hospitals was 5.6%, higher than that reported in the previous week (4.3%) and that in the corresponding period in 2015-2017 (2.7%, 3.0%, 2.7%). In northern provinces, that proportion was 4.5%, higher than those reported in the previous week (3.6%) and the corresponding period in 2015-2017 (2.7%, 3.3%, 2.7%). The proportion of influenza detections in the week ending Feb 18, 2018 was 33.0% (62.7% influenza A and 37.3% influenza B).
- In Macau (as of Feb 24, 2018), the influenza activity has slowed down but remained at high level. The proportions of ILI cases in emergency departments among adults and children decreased. The proportion of influenza detections was 37.6%, lower than 46.7% in the previous week.
- In Taiwan (week ending Mar 3, 2018), influenza activity remained at the peak of the season but was gradually slowing down. In the week ending Mar 3, the proportion of ILI cases in emergency department was 14.53% which was above the threshold of 11.4%. The predominating virus was influenza B.
- In Japan (week ending Feb 25, 2018), the influenza season has started in late November 2017. The average number of reported ILI cases per sentinel site has decreased to 22.64 in the week ending Feb 25, 2018 from 29.65 in the previous week. It was higher than the baseline level of 1.00. The predominating virus in the past five weeks was influenza B, followed by influenza A(H3N2) and A(H1N1)pdm09.