
#13,445
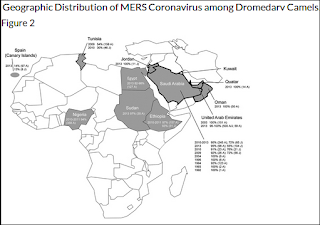
Not quite two months ago, in EID Journal: Geographic Distribution of MERS-CoV among Dromedary Camels, Africa, we looked (again) at the mystery of why MERS-CoV (or at least a very closely related MERS-like virus) has been found in camels across much of North Africa, and yet no human infections have been reported.
Today, a new study from Eurosurveillance finds no serological evidence of previous MERS infection among 261 presumably exposed camel abattoir workers in Nigeria.
We've seen previoiusly that mild MERS infection doesn't always leave long-lasting serological evidence behind (see EID Journal: Antibody Response & Disease Severity In HCW MERS Survivors), but a complete absence of positives is fairly striking.In 2016, in EID Journal: MERS-CoV Antibodies in Humans, Africa, 2013–2014, we looked at the results of a seroprevalence study conducted in Kenya, which found just two (weakly) positive samples out of blood samples collected from 1,122 livestock handlers in Kenya during 2013-2014.
The mystery continues, although it is quite possible that the Nigerian strain of MERS-CoV currently circulating in camels has less zoonotic potential than its Arabian Peninsula cousins.A link and some excerpts follow, but click the link to read the study in its entirety.
Lack of serological evidence of Middle East respiratory syndrome coronavirus infection in virus exposed camel abattoir workers in Nigeria, 2016
Ray TY So1,2, Ranawaka APM Perera1,2, Jamiu O Oladipo1,2,3, Daniel KW Chu1,2, Sulyman A Kuranga3, Kin-ho Chan1, Eric HY Lau1, Samuel MS Cheng1, Leo LM Poon1, Richard J Webby4, Malik Peiris1
Middle East respiratory syndrome coronavirus (MERS-CoV) is an ongoing threat to global public health [1]. Serological and virological studies have shown evidence of MERS-CoV infection in camels in the Middle East, as well as in East, North and West Africa [2-5] and in Central Asia [6].
In spite of MERS-CoV being enzootic in camels in Africa, zoonotic MERS has not been reported from the African continent. Our recent genetic and phenotypic analysis of MERS-CoV from camels in West (Burkina Faso, Nigeria) Africa has shown that West African viruses were phylogenetically and phenotypically distinct from those associated with human disease in the Arabian Peninsula [7], raising the possibility that virus strain differences may be associated with differences in zoonotic potential.
Abattoir workers with exposure to infected camels are a high-risk group for MERS-CoV infection in the Arabian Peninsula [8]. However, there is a paucity of serological data on MERS-CoV infection in people occupationally exposed to camels in Africa, a knowledge gap identified as a priority research question at a Food and Agriculture Organization of the United Nations-World Organisation for Animal Health-World Health Organization (FAO-OIE-WHO) Global Technical Meeting on MERS in September 2017 [1].
A previous study in Egypt in 2013 showed no serologic evidence of MERS-CoV among 179 serum samples from humans working in two camel abattoirs [3]. None of 760 people with household exposure to seropositive camels in Kenya in 2013 had evidence of MERS-CoV antibody [9]. Another study in Kenya in 2013–14 of 1,122 people (not with necessarily high exposure to camels) found two sera with low and inconclusive levels of neutralising antibody to MERS-CoV [10].
It remains important to carry out more sero-epidemiological studies on humans with occupational exposure to infected camels to understand whether or not zoonotic transmission is taking place in Africa. We therefore investigated for serological evidence of MERS-CoV infection of humans occupationally exposed to infected dromedary camels in an abattoir in Kano, Nigeria.
(SNIP)
In our study, of 261 workers exposed to camels in the abattoir in Kano, Nigeria, none were seropositive. This seropositivity rate is significantly lower than that of the camel abattoir workers in Saudi Arabia (p = 0.0049, Fisher’s exact test) and that of the camel barn workers at a race track in Qatar (p = 0.0058). The finding of only negative test results in 113 camel slaughterers in this study yields a significantly different rate of seropositivity than that in camel slaughterers in an animal market in Qatar (p = 0.0014). Our results are concordant with that of a study in Kenya, East Africa, where there was no evidence of antibody in serum of 760 people with household or occupational exposure to MERS-CoV seropositive camels [9].
(SNIP)
In conclusion, we found no serological evidence of MERS-CoV infection in abattoir workers with extensive exposure to dromedaries with documented virus infection in winter months. lt is possible that MERS-CoV from West Africa may have lower zoonotic potential than current virus strains in the Arabian Peninsula [7]. Studying MERS-CoV in humans in Africa is an urgent priority. There is also a need for additional studies to genetically and phenotypically characterise MERS-CoV in Nigeria and other parts of Africa.
(Continue . . . )