
#13,552
We've been following the C. auris story since June of 2016 when the CDC issued a Clinical Alert to U.S. Health care facilities about the Global Emergence of Invasive Infections Caused by the Multidrug-Resistant Yeast Candida auris.
C. auris is an emerging fungal pathogen that was first isolated in Japan in 2009. It was initially found in the discharge from a patient's external ear (hence the name `auris'). Retrospective analysis has traced this fungal infection back over 20 years.Since then the CDC and public health entities have been monitoring an increasing number of cases (and hospital clusters) in the United States and abroad, generally involving bloodstream infections, wound infections or otitis.
Adding to the concern:We've the latest CDC monthly update, along with brief looks at two recent studies published in the CDC's EID Journal.
- C. auris infections have a high fatality rate
- The strain appears to be resistant to multiple classes of anti-fungals
- This strain is unusually persistent on fomites in healthcare environments.
- And it can be difficult for labs to differentiate it from other Candida strains
More than half (n= 223 of 397) of all confirmed C. auris infections in the United States have been identified in New York State, which appropriately is the focus of the first EID study:
Volume 24, Number 10—October 2018
Research
Candida auris in Healthcare Facilities, New York, USA, 2013–2017
Eleanor Adams, Monica Quinn, Sharon Tsay, Eugenie Poirot, Sudha Chaturvedi, Karen Southwick, Jane Greenko, Rafael Fernandez, Alex Kallen, Snigdha Vallabhaneni, Valerie Haley, Brad Hutton, Debra Blog, Emily LutterlohComments to Author , Howard Zucker, and Candida auris Investigation Workgroup1
Abstract
Candida auris is an emerging yeast that causes healthcare-associated infections. It can be misidentified by laboratories and often is resistant to antifungal medications.
We describe an outbreak of C. auris infections in healthcare facilities in New York City, New York, USA. The investigation included laboratory surveillance, record reviews, site visits, contact tracing with cultures, and environmental sampling. We identified 51 clinical case-patients and 61 screening case-patients. Epidemiologic links indicated a large, interconnected web of affected healthcare facilities throughout New York City.
Of the 51 clinical case-patients, 23 (45%) died within 90 days and isolates were resistant to fluconazole for 50 (98%). Of screening cultures performed for 572 persons (1,136 total cultures), results were C. auris positive for 61 (11%) persons. Environmental cultures were positive for samples from 15 of 20 facilities. Colonization was frequently identified during contact investigations; environmental contamination was also common.(Continue . . .)
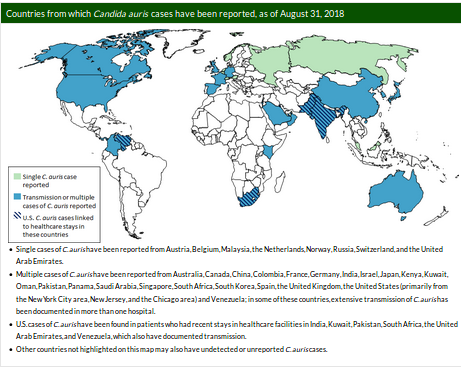
As depicted the the following CDC map, C. auris is very much a global problem, although limited surveillance prevents us from knowing just how widespread this fungal infection really is.
Today's second EID Journal report focuses on C. auris in South African hospitals.
Research
Candida auris in South Africa, 2012–2016
Nelesh P. Govender, Rindidzani E. Magobo, Ruth Mpembe, Mabatho Mhlanga, Phelly Matlapeng, Craig Corcoran, Chetna Govind, Warren Lowman, Marthinus Senekal, and Juno Thomas
Abstract
To determine the epidemiology of Candida auris in South Africa, we reviewed data from public- and private-sector diagnostic laboratories that reported confirmed and probable cases of invasive disease and colonization for October 2012–November 2016.
We defined a case as a first isolation of C. auris from any specimen from a person of any age admitted to any healthcare facility in South Africa. We defined probable cases as cases where the diagnostic laboratory had used a nonconfirmatory biochemical identification method and C. haemulonii was cultured. We analyzed 1,692 cases; 93% were from private-sector healthcare facilities, and 92% of cases from known locations were from Gauteng Province. Of cases with available data, 29% were invasive infections.And finally, the September update from the CDC, which adds 36 new confirmed cases to the previous month's total, bring the total confirmed and probable US cases to 427.
The number of cases increased from 18 (October 2012–November 2013) to 861 (October 2015–November 2016). Our results show a large increase in C. auris cases during the study period, centered on private hospitals in Gauteng Province.
(Continue . . . )
Additionally, based on targeted screening in just four of the states which have reported clinical cases, the CDC reports an additional 743 patients have been discovered to be asymptomatically colonized with C. auris.
September 28, 2018: Case Count Updated as of August 31, 2018
Candida auris is an emerging fungus that presents a serious global health threat. C. auris causes severe illness in hospitalized patients in several countries, including the United States. Patients can remain colonized with C. auris for a long time and C. auris can persist on surfaces in healthcare environments. This can result in spread of C. auris between patients in healthcare facilities.
Most C. auris cases in the United States have been detected in the New York City area, New Jersey, and the Chicago area. Strains of C. auris in the United States have been linked to other parts of the world. U.S. C. auris cases are a result of inadvertent introduction into the United States from a patient who recently received healthcare in a country where C. auris has been reported or a result of local spread after such an introduction.
Candida auris was made nationally notifiable at the 2018 Council for State and Territorial Epidemiologists (CSTE) Annual Conference. For the updated case definition and information on the nationally notifiable condition status, which will go into effect in 2019, please see the 2018 CSTE position statement[PDF – 16 pages].

CDC encourages all U.S. laboratories that identify C. auris to notify their state or local public health authorities and CDC at candidaauris@cdc.gov. CDC is working closely with public health and healthcare partners to prevent and respond to C. auris infections. The CDC-sponsored Antibiotic Resistance Laboratory Network (ARLN) will help improve detection and response to C. auris nationwide.