#17,385

Although COVID (aka SARS-CoV-2) seemingly came out of the blue in Wuhan China in December of 2019 - and has since sparked the worst pandemic in 100 years - researchers had been closely monitoring a number of similar coronaviruses from around the globe since the early 2000s.
The original SARS-CoV virus, which went on a limited world tour in 2002-2003 (see SARS and Remembrance), was our first indication that a coronavirus could produce severe, even fatal, illness in humans.
Following the SARS-CoV outbreak, a number of other coronaviruses were detected in bats around the world, but most appeared to pose only a low risk of infecting humans. That changed in the summer of 2012 when we learned of the first known infection by a new coronavirus in Saudi Arabia that would eventually be dubbed MERS-COV.
Only later would we learn there had been a deadly hospital outbreak months earlier in Jordan.
But at the time, the virus was unknown, and it would take nearly 2 years of retrospective investigation before the full extent of that outbreak would be revealed (see Serological Testing Of 2012 Jordanian MERS Outbreak).
The (likely intermediate) host for MERS-CoV was determined to be camels in the fall of 2013, although a number of other mammals appear to be susceptible as well (see Nature: Comparative Susceptibility of SARS-CoV-2, SARS-CoV, and MERS-CoV Across Mammals).
Between 2012 and 2020, more than 2,000 human infections were recorded, mostly from the Middle East. But in 2015 in South Korea, a single infected traveler sparked an epidemic which eventually infected 185 people across 16 hospitals, and claimed 38 lives (see Superspreaders & The Korean MERS Epidemiological Report).
Prior to 2020 MERS-CoV was considered a legitimate pandemic threat, and while SARS-CoV-2 beat it to the punch, it remains a genuine concern.
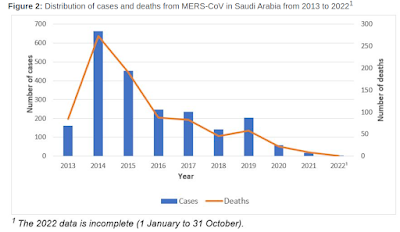
While the number of MERS-CoV cases reported out of the Middle East has plummeted over the past 3 years (see Saudi Epi chart below), there are strong suspicions that has more to do with a lack of surveillance and reporting than any disappearance of the virus.
In last November's Update: Middle East Respiratory Syndrome Coronavirus (MERS-CoV) – Saudi Arabia, the World Health Organization cautioned:
The number of MERS-CoV cases reported to WHO has substantially declined since the beginning of the ongoing COVID-19 pandemic. This is likely the result of epidemiological surveillance activities for COVID-19 being prioritized, resulting in reduced testing and detection of MERS-CoV cases.But even before the COVID pandemic, we'd seen estimates that the vast majority of MERS cases go undiagnosed (or unreported) in the Middle East (see EID Journal: Estimation of Severe MERS Cases in the Middle East, 2012–2016).
Less than two weeks ago we looked at the (theoretical) potential for SARS-CoV-2 and MERS-CoV to recombine into a hybrid virus (see Nature: CoV Recombination Potential & The Need For the Development of Pan-CoV Vaccines).
Even without such an untoward event, MERS-CoV is quite capable of evolving on it own.
All of which brings us to an excellent review, and analysis, of the the spread and evolution of MERS-CoV in camels and humans over the past decade, published last week in the International Journal of Infectious Diseases.
This is a lengthy and detailed report, with much of it of interest primarily to virologists. I've only posted some excerpts, so follow the link if you wish to read the full study.
I'll have a brief postscript when you return.
Middle East Respiratory Syndrome Coronavirus (MERS-CoV) – a ten-year (2012-2022) global analysis of human and camel infections, genomic sequences, lineages, and geographical origins
Esam I Azhar 1 *, Thirumalaisamy P Velavan 2 *, Ikrormi Rungsung 2, Tieble Traore 3, David S Hui 4, Brian McCloskey 5, Sherif A El-Kafrawy 1 *, Alimuddin Zumla
Highlights
- MERS-CoV remains on the WHO priority pathogens list
- WHO reports 2,184 out of a total of 2591 human MERS cases are from Saudi Arabia
- Three MERS-CoV Clades were identified: Clade B(n=462), clade A(n=10), clade C(n=5)
- New MERS-CoV variants and co-infections continue to circulate in camels
- Proactive virus surveillance and genomic analyses in camels and humans is required
Abstract
Background
The WHO priority zoonotic pathogen MERS-CoV has a high case fatality rate in humans and circulates in camels worldwide.
Methods
We performed a global analysis of human and camel MERS-CoV infections, epidemiology, genomic sequences, clades, lineages and geographical origins for the period January 1st, 2012, to August 3rd, 2022. MERS-CoV ‘S’-gene sequences (4061bp) were extracted from Genebanks, and a phylogenetic maximum likelihood tree constructed.
Findings
As of August 2022, 2591 human MERS cases from 26 countries were reported to the WHO (Saudi Arabia, 2184 cases, including 813 deaths (CFR:37.2%) Whilst declining in numbers, MERS cases continue to be reported from the Middle East. 728 MERS-CoV genomes identified (the largest number were from Saudi Arabia:222:human=146, camels=76) and UAE(176:human=21,camels=155). 501 ‘S’-gene sequences were used for phylogenetic tree construction [camels(n=264), humans(n=226), bats(n=8), other(n=3)]. Three MERS-CoV Clades were identified: the largest, Clade B, followed by clade A and clade C. Of 462 Clade B lineages, lineage 5 was predominant,(n=177).
Interpretation
MERS-CoV remains a threat to global health security. MERS-CoV variants continue circulating in humans and camels. Recombination rates indicate co-infections with different MERS-CoV lineages. Proactive surveillance of MERS-CoV infections and variants of concern in camels and humans worldwide is essential for epidemic preparedness.
Introduction
Three novel coronaviruses (CoV) have emerged over the past two decades causing lethal diseases in humans: The Severe Acute Respiratory Syndrome (SARS) coronavirus (SARS-CoV-1) [1,2], the Middle East Respiratory Syndrome (MERS) Coronavirus (MERS-CoV) [3-7], and more recently SARS-CoV-2 [8,9]. In 2002, SARS-CoV-1 jumped species from civet cats to humans, and rapidly spread by human-to-human transmission across continents, causing 8098 cases and 774 deaths (9.6% case fatality rate-CFR) [1,2]. It disappeared within 18 months and no human cases of SARS-CoV-1 infection have been recorded since January 2004 [1].
SARS-CoV-2 was first reported in December 2019 from Wuhan, Hubei province in China,[8,9], and subsequently spread worldwide causing the unprecedented pandemic of Coronavirus Disease-2019 (COVID-19) with a case fatality rate of 1.1% [9]. The emergence of genetic variants of concern (VOC) in SARS-CoV-2 has generated serious dialogue regarding the evolution of new genotypes, transmissibility, and response to vaccines [9].
MERS-CoV was first detected in clinical samples of a patient with pneumonia who died in a Jeddah hospital, in Saudi Arabia in 2012 [3]. Since then, over 2,500 cases of laboratory-confirmed MERS cases have been reported from 27 countries, with a high case-fatality ratio (CFR) of up to 35%) [4,5,6]. MERS-CoV has been identified in dromedary camels in the Middle East, Africa and South Asia [4,5]. Exposure to dromedaries is recognized as a risk factor for primary human MERS cases [4-7].
Recombination in coronaviruses is of great evolutionary importance since it is associated with expansion in host range, transmissibility, global spread changes in pathogenicity and host response [10]. Although MERS-CoV is associated with a high mortality rate, and it remains on the WHO blueprint list of priority pathogens, scientific and political attention on it has been eclipsed by the unprecedented SARS-CoV-2 (COVID-19) pandemic. As with SARS-COV-2 [9], new MERS-CoV lineages and variants with more or less efficient transmission capabilities may emerge over time. The large, unexpected large MERS-CoV outbreak in South Korea in 2015 highlighted the epidemic potential of MERS-CoV [10-13].
MERS-CoV continues to circulate in camels and humans, remaining a threat to global health security [4-6,15-25]. Information on the evolution of MERS-CoV lineages, clades and new variants in humans and animals remains scanty and major knowledge gaps remain. Thus, similar to the collective global efforts at genomic sequencing and surveillance of SARS-CoV-2 variants [9], increasing surveillance, genomic sequencing and monitoring of MERS-CoV circulation in camels and humans are equally important. We performed a ten-year (2012-2022) analysis of MERS-CoV infections, epidemiology, sequences, lineages, clades, animal host and geographical origins.
(SNIP)
Conclusions
MERS-CoV remains a threat to global health security. Whilst numbers of human MERS cases have declined over the past 5 years, new MERS-CoV variants continue to circulate in camels and humans. Recombination rates indicate co-infections with different MERS-CoV lineages, and adaptive potential in camels. Proactive surveillance of MERS-CoV infections and variants of concern in camels and humans worldwide is essential for epidemic preparedness. MERS-CoV remains a WHO priority pathogen and further research and investments are required to understand MERS-CoV evolution and circulation in dromedary camels and to limit spillover infections to humans. Heightened vigilance and surveillance should be in place in lieu of the huge camel MERS-CoV reservoir.
Potential For Zoonotic Emergence Of Coronavirus In Latin America
EID Journal: A New Bat-HKU2–like Coronavirus in Swine, China, 2017
Emerg. Microbes & Infect.: Novel Coronaviruses In Least Horseshoe Bats In Southwestern China
Whether front and center, or obscured by the fog of COVID, all of these threats (and many others like them) are still out there, quietly doing what viruses do best; evolving, spreading, and looking for new hosts.