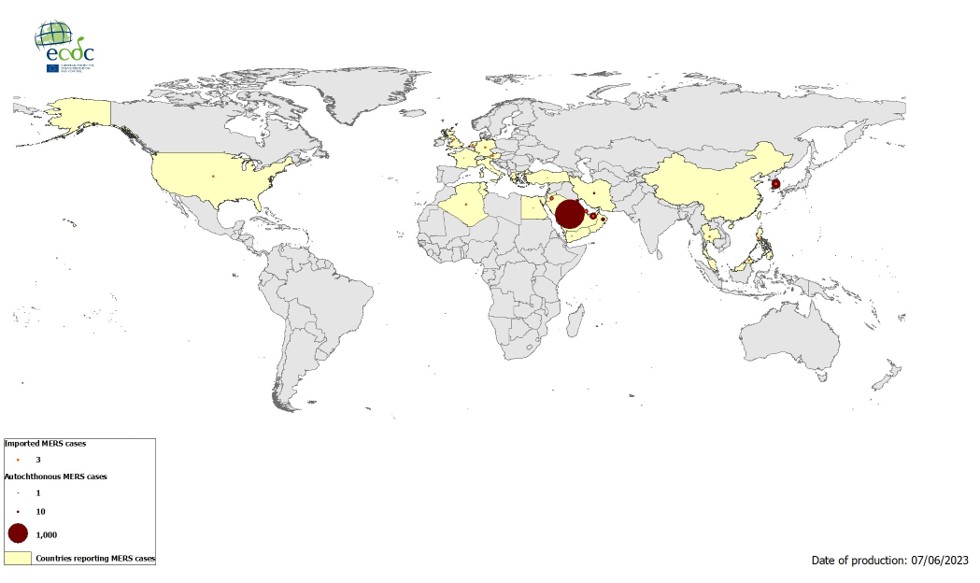
Geographical distribution of confirmed cases of MERS-CoV, by reporting country, April 2012 – May 2023 - EN - [JPG-69.04 KB]
#17,506
With the first unrestricted Hajj since the emergence of COVID-19 scheduled to run from Monday June 26th to Saturday July 1st - and as many as 2 million religious pilgrims from around the world expected to attend - we are once again seeing attention focused on another coronavirus threat; MERS-CoV.
Over the past month we've seen the UKHSA Issue Hajj Travel Advice On MERS-CoV and in another blog a WHO sponsored EPI-WIN webinar titled: MERS-CoV, a circulating coronavirus with epidemic and pandemic potential - Pandemic preparedness, prevention and response with a One Health approach.
While MERS-CoV isn't anywhere near as transmissible as SARS-CoV-2, it has sparked large nosocomial outbreaks in the past, and it tends to be far deadlier (based on known cases) than COVID. The good news is, reports of MERS-CoV infections have plummeted since 2019.

The number of MERS-CoV cases reported to WHO has substantially declined since the beginning of the ongoing COVID-19 pandemic. This is likely the result of epidemiological surveillance activities for COVID-19 being prioritized, resulting in reduced testing and detection of MERS-CoV cases.
Even when countries are aggressively looking for cases, detecting MERS-CoV cases can be difficult, and official case counts are thought to be significant under counts (see EID Journal: Estimation of Severe MERS Cases in the Middle East, 2012–2016. Some past blogs on these challenges include:
EID Journal: Sensitivity and Specificity Of MERS-CoV Antibody Testing
AJIC: Intermittent Positive Testing For MERS-CoV
JIDC: Atypical Presentation Of MERS-CoV In A Lebanese Patient
Since MERS-COV emerged on the Arabian peninsula in 2012, it has been viewed as having some pandemic potential of its own (see 2017's A Pandemic Risk Assessment Of MERS-CoV In Saudi Arabia), meaning it doesn't necessarily need a viral co-conspirator to pose a threat.
UKHSA risk Asessment of MERS-CoV
Updated 23 June 2023
Epidemiological update
As of June 2023, over 2,600 cases of Middle East Respiratory Syndrome (MERS-CoV) have been reported by the World Health Organization (WHO). The majority of MERS-CoV cases have been reported from the Arabian Peninsula, with one large outbreak outside this region involving 186 cases in the Republic of Korea (RoK) in 2015. Cases have been exported to other countries outside of the Middle East, including cases being identified in the UK and South Korea in August and September 2018 respectively.
On 22 August 2018, Public Health England (PHE) – now the UK Health Security Agency (UKHSA) – reported a laboratory-confirmed case of MERS-CoV infection in a resident of the Middle East who had travelled from Saudi Arabia. In response to this, public health measures were implemented including identification of exposed contacts and provision of health advice. This was the third imported MERS case reported by the UK; the previous case was reported in 2013 was associated with 2 infections in close contact.
Excluding the 2015 outbreak in RoK, the majority of reported cases of MERS-CoV worldwide have been from the Kingdom of Saudi Arabia (KSA).
MERS-CoV in Saudi Arabia
In KSA, cases of MERS-CoV occur throughout the year. There is currently no evidence of sustained community transmission; human-to-human transmission is most likely to occur in healthcare facilities and household clusters. Large outbreaks linked to healthcare facilities are a feature of MERS-CoV and have occurred both within the Middle East and RoK. This underlines the significance of healthcare facilities as a risk factor for amplifying infection, but also the importance of effective and rapid implementation of infection prevention and control practices for possible cases to limit the potential for onward transmission to other patients and staff.
Outside of hospital outbreaks and smaller household clusters, reported cases are sporadic and usually occur in individuals with a history of contact with camels or camel products such as consumption of raw camel milk. UKHSA will continue to monitor the situation internationally.
Risk assessment
The previous sporadic imported cases to the UK highlight the continued risk of imported cases to the UK, reflecting the epidemiology of MERS-CoV infection in the Middle East. It is therefore imperative that health professionals remain vigilant for clinical presentations compatible with Middle East Respiratory Syndrome. Early identification and rapid implementation of appropriate infection control measures for possible cases, and reporting of these to local health protection teams is crucial.
The risk of infection with MERS-CoV to UK residents in the UK remains very low.
The risk of infection with MERS-CoV to UK residents travelling to the Middle East is very low, but may be higher in those with exposure to specific risk factors within the region, such as camels (or camel products) or the local healthcare system.
Testing for MERS-CoV is warranted for persons who meet the possible case definition together with rapid implementation of appropriate infection control measures while awaiting results of testing.
The majority of outbreaks of MERS-CoV in the Middle East have been linked to healthcare settings. A previous WHO mission to Saudi Arabia concluded that gaps in infection control measures have most likely contributed to these outbreaks; this reinforced the importance of strict adherence to recommended infection control measures in healthcare facilities.
Where UK infection control procedures have been followed, the probability of acute respiratory infection in a healthcare worker caring for a case of MERS-CoV, or a case of severe acute respiratory infection of unknown aetiology in the intensive care unit (ICU), being due to MERS-CoV is very low, but warrants testing. Any healthcare worker who develops an acute respiratory illness and has recently been in contact with a confirmed case of MERS-CoV would be tested for the virus. The risk will be higher for healthcare workers exposed to MERS-CoV who have not adhered to UK infection control procedures, such as the use of adequate personal protective equipment (PPE).
The risk to contacts of confirmed cases of MERS-CoV infection is low, but contacts should be followed up for 14 days following last exposure and any new febrile or respiratory illness investigated urgently for MERS-CoV.
Further information and guidance on MERS-CoV is available.
Travel adviceThe Hajj and Umrah
- All travellers to the Middle East are advised to avoid contact with camels as much as possible:travellers should practice good general hygiene measures, such as regular handwashing with soap and water at all times, but especially before and after visiting farms, barns or market areas
- travellers are advised to avoid raw camel milk and/or camel products from the Middle East
- travellers are also advised to avoid consumption of any type of raw milk, raw milk products and any food that may be contaminated with animal secretions unless peeled and cleaned and/or thoroughly cooked
- travellers should follow the advice of local health authorities; there are currently no travel restrictions in place
- travellers developing fever and cough within 14 days of travel from the Middle East should seek medical advice and must report their travel history so that appropriate clinical assessment, infection control measures and testing can be undertaken
- people who are acutely ill with an infectious disease are advised not to travel but to seek health advice immediately
International pilgrims will be allowed to undertake the Hajj in 2023, with significant numbers of pilgrims expected to attend, and no upper age limitations.
The last Hajj where such numbers of international pilgrims could attend was in 2019. There was no reported increase in travel-related MERS-CoV cases for this latest or previous Hajj pilgrimages. However, cases of MERS-CoV have been imported to countries outside of Saudi Arabia following return from Umrah, a separate pilgrimage which can be performed throughout the year, as illustrated by the most recent Malaysian case.
UKHSA remains vigilant and closely monitors developments in the Middle East and in the rest of the world where new cases have emerged and continues to liaise with international colleagues to assess whether our recommendations need to change.
Infographics for people travelling to the Middle East or returning from the Middle East are available in a range of languages.
NaTHNaC has published travel health advice for Hajj and Umrah.
Further information for health professionals on the possible MERS case definition is available.
While the risks of seeing exported cases of MERS-CoV following the Hajj are believed low, they are not zero. Public health officials around the world will need to be on heightened alert for exported cases for several weeks after the Hajj ends.
But MERS-CoV is far from the only concern.
Mass gatherings provide target rich environments for viruses, bacteria, and other pathogens (e.g. influenza, RSV, Scarlet Fever, measles, emerging COVID variants, Dengue, etc.), and modern air travel allows people to return home well within the incubation period.
The reality of life in 21st century is that disease threats that once were local, can now spread globally in a matter of hours or days. Vast oceans and prolonged travel times no longer protect us against infected travelers crossing borders.