
#16,676
Long-time readers of this blog are aware that the flow of information out of Saudi Arabia on MERS-CoV cases has been erratic at best over the past 10 years. We've often gone long periods without updates, and we've seen instances where the Saudi MOH - after saying nothing for months - will `backfill' dozens of previously unannounced cases.
The Saudi MOH MERS-CoV landing page (see below), hasn't been updated since Epi Week 2 of 2022 (1/15/22), and no case detail page has been setup for 2022 (see 2021 page).

Until the pandemic began, we usually saw WHO updates from Saudi Arabia at least once a month, and while it was understood that surveillance was likely only picking up a fraction of actual cases (see EID Journal: Estimation of Severe MERS Cases in the Middle East, 2012–2016), it at least gave us some idea of the trajectory of the virus in the region.
Since the pandemic began, reporting of MERS-Cases has plummeted (see WHO EMRO Chart below). Whether this reflects a genuine drop in MERS cases, or changes in surveillance and reporting isn't clear.

Today the WHO has published what they are calling `the bi-annual update on Middle East Respiratory Syndrome Coronavirus', which sadly, suggests that more frequent updates are probably not expected any time soon.
Middle East respiratory syndrome coronavirus (MERS-CoV) – Saudi Arabia7 April 2022
Summary
This is the bi-annual update on Middle East Respiratory Syndrome Coronavirus (MERS-CoV) infections reported to WHO from the Kingdom of Saudi Arabia. Between 1 August 2021 to 28 February 2022, six additional cases of MERS-CoV infections, including four associated deaths were reported to WHO from the Kingdom of Saudi Arabia. These cases were reported from Riyadh (four cases), Eastern (one case), and Taif (one case) regions. Based on the current situation and available information, WHO re-emphasizes the importance of strong surveillance by all Member States for acute respiratory infections, including MERS-CoV, and careful review of any unusual patterns.
Description of cases
Since the last Disease Outbreak News on MERS-CoV in Saudi Arabia published on 17 August 2021, the National IHR Focal Point of Saudi Arabia has reported six additional cases, including four associated deaths. The geographical distribution of these reported cases is shown in Figure 1.

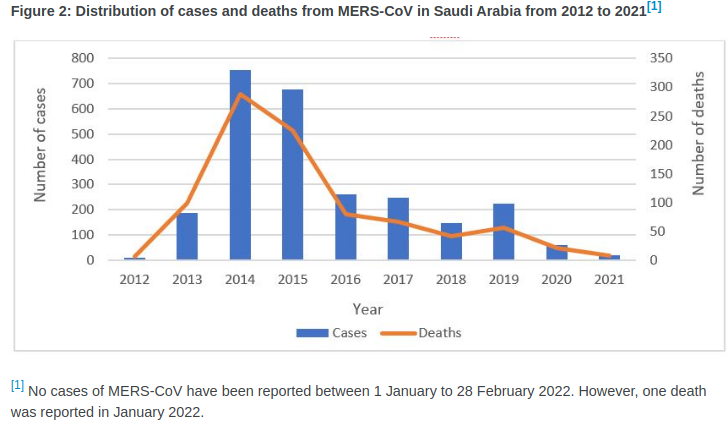
Between September 2012 and 28 February 2022, a total of 2585 cases, including 891 associated deaths (case fatality rate: 35%) have been globally reported to WHO under the International Health Regulations (IHR 2005) (Figure 2). The majority of these cases have occurred in countries in the Arabian Peninsula, with one large outbreak outside this region in May 2015, when 186 laboratory-confirmed cases (185 in the Republic of Korea and one in China) and 38 deaths were reported.
Figure 2: Distribution of cases and deaths from MERS-CoV in Saudi Arabia from 2012 to 2021[1]
(SNIP)
WHO risk assessment
The notification of the six cases does not change the overall risk assessment. WHO expects that additional cases of MERS-CoV infection will be reported from the Middle East and/or other countries where MERS-CoV is circulating in dromedary camels, and that cases will continue to be exported to other countries by individuals who were exposed to the virus through contact with dromedary camels or their products (for example, consumption of camel’s raw milk), or in a healthcare setting. WHO continues to monitor the epidemiological situation and conducts risk assessment based on the latest available information.
The number of MERS-CoV cases reported to WHO has substantially declined since the beginning of the ongoing COVID-19 pandemic (Figure 2). This is likely the result of epidemiological surveillance activities for COVID-19 being prioritized, resulting in reduced testing and detection of MERS-CoV cases. The Ministry of Health of Saudi Arabia continues to work to improve testing capacities for better detection of MERS-CoV during the ongoing COVID-19 pandemic.
To be fair, we aren't hearing much from other nations on the Arabian peninsula, where MERS-CoV has also been been detected in both camels and humans. And it seems likely that cases are being missed in North and Central Africa as well (see EID Journal: Geographic Distribution of MERS-CoV among Dromedary Camels, Africa).

Over the past decade we've looked at many of the challenges of MERS-CoV surveillance, including:
EID Journal: Sensitivity and Specificity Of MERS-CoV Antibody Testing
AJIC:Intermittent Positive Testing For MERS-CoV
JIDC: Atypical Presentation Of MERS-CoV In A Lebanese Patient
And in 2018 - in Evaluation of a Visual Triage for the Screening of MERS-CoV Patients - we looked at a highly critical review of the screening methods used by the Saudis for selecting patients for MERS testing. As a result, the official total of 2585 cases is highly suspect.
While MERS-CoV hasn't embarked on a world tour the way that SARS-CoV-2 has, we've seen studies (see A Pandemic Risk Assessment Of MERS-CoV In Saudi Arabia) suggesting the virus doesn't have all that far to evolve before it could pose a genuine global threat.As is the Saudi's detection of only 6 human infections over the past 6 months.
So while it is possible that the MERS threat has receded greatly, and this virus is rarely jumping to humans.