![]()
#17,002
Although reports of human infection with avian influenza (H5N6, H9N2, and H3N8) by China have dropped precipitously since the spring there are strong reasons to believe that zoonotic HPAI viruses are still circulating in wild birds and poultry on the Mainland (EID Journal: Novel Zoonotic Avian Influenza Virus A(H3N8) Virus in Chicken, Hong Kong, China).
What China lacks in real time reporting they often make up for with solid research articles, and over the summer we've continued to see a steady stream of cautionary reports published in international scientific journals, including:
Preprint: Human infection With a Novel Reassortment Avian Influenza A H3N8 Virus: An Epidemiological Investigation Study
Study: Adaptation of Two Wild Bird-Origin H3N8 Avian Influenza Viruses to Mammalian Hosts
The constant across all of these reports is that the avian flu threat in China continues to evolve, and not in a good way. H3N8 has recently been shown to be zoonotic, H5N6 continues diversify into new, more dangerous clades, and H9N2 remains a player, providing the genetic `backbone' for many of these reassortant viruses.
While influenza viruses (including avian flu) generally produce respiratory infections, they can occasionally produce severe neurological manifestations (see 2018's Neuroinfluenza: A Review Of Recently Published Studies).
Over the past year we've seen an increasing number of reports of avian H5N1 clade 2.3.4.4b - which is currently circulating in wild birds and poultry in Europe and North America - infecting mammals (seals, dolphins, foxes, bears, etc.) and producing profound neurological symptoms (see here, here, here, and here).
These reports are reminiscent of past reports regarding the HPAI Asian H5N1 virus, including:
- In 2009, a PNAS study (link below) found that the H5N1 virus was highly neurotropic in lab mice, and in the words of the authors `could initiate CNS disorders of protein aggregation including Parkinson's and Alzheimer's diseases’.
- In 2015, after the death of the first imported H5N1 case in Canada, we saw a study (see CJ ID & MM: Case Study Of A Neurotropic H5N1 Infection - Canada), where the authors wrote: `These reports suggest the H5N1 virus is becoming more neurologically virulent and adapting to mammals'.
- In a Scientific Reports study on the genetics of the H5N1 clade 2.3.2.1c virus - Highly Pathogenic Avian Influenza A(H5N1) Virus Struck Migratory Birds in China in 2015 – the authors warned of its neurotropic effects, and that it could pose a ` . . . significant threat to humans if these viruses develop the ability to bind human-type receptors more effectively.'
I've only included abstract, and excerpts from the discussion, so you'll want to follow the link to read it in its entirety.
Research Article
Clinical features of the first critical case of acute encephalitis caused by avian influenza A (H5N6) virus
Libing Zhang, Kaituo Liu, Qin Su, Xiao Chen, Xiaoquan Wang, Qingfeng Li, show all
Accepted author version posted online: 12 Sep 2022
Download citation
https://doi.org/10.1080/22221751.2022.2122584
Abstract
Highly pathogenic avian influenza virus (HPAIV) such as H5N1, H5N6, and H7N9 have been reported to frequently infect human, but acute encephalitis caused by HPAIV in human have been rarely reported. We report the first critical case of acute encephalitis with mild pneumonia caused by H5N6 virus. On January 25 of 2022, a 6-year-old girl with severe neurological symptoms was admitted to our hospital and rapidly developed to seizures and coma. Brain imaging showed abnormalities.Electroencephalogram (EEG) presented abnormal slow waves. Cerebrospinal fluid (CSF) contained elevated protein (1.64 g/L) and white cells (546×106/L). Laboratory investigations revealed abnormally elevated transaminases, lactate dehydrogenase and cytokines in serum. A novel reassortant H5N6 virus was identified from the patient’s serum, CSF and tracheal aspirate specimens. Phylogenic analysis indicated that this virus was a novel reassortant avian-origin influenza A (H5N6) virus belonged into clade 2.3.4.4b.This patient was diagnosed with acute encephalitis and discharged from the hospital accompanied with language barrier. Epidemiological investigation confirmed that wild waterfowls were the direct source of infection of this case. Our study highlights the urgent need to pay attenuation to acute encephalitis caused by HPAIV.
Introduction
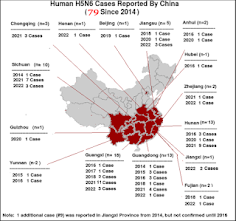
Due to the high lethality to humans, highly pathogenic avian influenza virus (HPAIV) such as H5N1, H7N9, and H5N6 have posed a great threat to human health [1-3]. During the past 20 years, H5N1 virus has caused a total of 863 cases including 455 deaths in the world [4]. However, since 2014, H5N6 reassortant virus have been circulating in poultry and occasionally infected humans in China [3, 5].
To date, a total of 78 cases (32 deaths) of H5N6 virus have been reported, of which 77 cases occurred in China [6]. Notably, most cases of H5N6 infection occurred in 2021 and 2022 [5-8]. Different from seasonal influenza, most of patients infected with HPAIV presented primarily with severe respiratory symptoms, neurological symptoms associated with acute encephalitis in human are still extremely rare.
Here, we report the first critical case of acute encephalitis diagnosed by identifying the H5N6 virus from cerebrospinal fluid (CSF), throat, and serum specimens in a 6-year-old girl who presented with seizures and coma. The clinical features of the patient with acute encephalitis are described and the epidemiological investigation was established. She was discharged from the hospital, but brain imaging and electroencephalogram (EEG) still indicated abnormalities. All evidence indicated the most likely resource of infection might be the wild-waterfowl. Our study highlights that attention needs to be paid to viral encephalitis caused by HPAIV (H5N6) transmitted by migratory birds.
(SNIP)
Discussion
Influenza A virus is primarily limited to the respiratory system, but many of the reported cases of influenza A virus including the “1918 H1N1” influenza pandemic had neurological symptoms typical of encephalitis, which can result in severe neurological sequelae and even death [33, 34]. Influenza-associated encephalitis and encephalopathy (IAE) caused by influenza A H3N2 or H1N1 is most frequently reported in children although adults cases are described [34, 35].
However, acute neurological symptoms from mild encephalitis to motor disturbances to coma caused by HPAIV have been observed mainly in poultry and wild mammals [36, 37]. In addition, most patients infected by HPAIV including H5N1, H5N6, and H7N9 exhibit primarily with acute respiratory illness, rare neurological symptoms have been reported [1-3]. To date, there are only 3 case reports of H5N1 infections with encephalitis, but only one fatal case was confirmed by isolating of H5N1 virus from the stored CSF [38, 39]. However, due to no increase in white cells in CSF and the lack of brain imaging, it cannot conclusively determine whether the patient had true encephalitis [39]. Virological diagnosis are a prerequisite for determining whether AIE occurs.
To our best knowledge, most reports of IAE were mainly based on the detection of influenza A virus RNA from CSF, rare evidence of isolating influenza A virus [33, 34]. In addition, excessive cytokine storm was observed in most patients with IAE[33]. Therefore, the current prevailing theory is that IAE might be associated with hypercytokinemia rather than actual viral invasion. However, the pathogenic mechanisms of IAE remains largely unknown. In this study, our results clearly indicated that the patient’s acute encephalitis was caused by H5N6 virus infection.
The diagnosis of acute encephalitis was based on the following evidences: neurological symptoms, brain imaging, EEG, biochemical characteristics of CSF and serum specimens, serology analysis, and virus isolation. The virological diagnosis was confirmed by RT-PCR, mNGS, and virus isolation from serum, CSF, and throat-swab specimens. Due to the identification of pathogen in all clinical specimens were performed by different staff on separate places at different dates apart (Yangzhou Center for Disease Control and Prevention, Vision Medicals Co. Ltd (Guangzhou, China), and Yangzhou University), the possibility of laboratory contamination can be completely ruled out. Ongoing in vivo work will reveal the potential pathogenesis of viral encephalitis caused by this virus.
In previously reported cases of IAE, clinical symptoms of influenza include but are not limited to fever, headache, pharyngitis, myalgia [33, 34, 40]. For this particular patient, she had symptoms of fever, headache, dizziness, vomiting, walking instability, language reduction, and sleep increase with elevated white cells and neutrophils, but had no obvious respiratory symptoms on illness onset. Therefore, it may be suspected as bacterial infection on illness onset. However, after 5 days of antibiotic treatment, not only did her symptoms not improve significantly, but instead rapidly progressed to typical symptoms of encephalitis, such as convulsions, epilepsy and coma. Therefore, acute encephalitis was suspected, and antiviral therapy was given empirically with acyclovir. After diagnosis of H5N6 virus infection, the patient was changed to peramivir treatment.
In previous literatures, steroid pulse therapy in the acute phase of IAE has beneficial effects on patient’s morbidity and mortality [41, 42]. In view of excessive cytokines storms in sera, she received steroid pulse therapy with methylprednisolone. In addition, our experience suggests that the specialized supportive therapies of PICU including mechanical ventilation, early convulsion control, reduction of cranial pressure and edema, anti-epileptic treatment, fluid management, and nutritional support may play an important role in the improvement of the prognosis of this case. Therefore, our research will provide a reference for clinicians, virologists, and public health experts to guide clinical treatment, laboratory diagnosis and epidemiological surveillance for this potential pandemic disease.
Due to the patient’s family neither raised poultry nor slaughtered poultry, the possibility of exposure to ill poultry should be ruled out. Moreover, long-term epidemiologic surveillance from our lab indicated that there was no this novel H5N6 reassortant circulating in poultry in Yangzhou city. Additionally, there were large amounts of wild waterfowl and domestic ducks living together in the inner lake in front of the patient’ house, we speculate that the most likely source of transmission might be wild waterfowl overwintering in the lake.The above speculation is further supported by the latest epidemiological reports, suggesting that these novel H5N6 reassortants including A/Hangzhou/1/2021 and A/duck/Zhejiang/S4854/2021, which are most closely related with YZ125 virus, may be generated through reassortment between migratory wild birds and domestic ducks. Recently, we isolated one H5N6 virus shared with highly homologous to YZ125 (H5N6) virus from the feces of wild waterfowl where the patient live, further confirming the above speculation. Moreover, it is worth noting that this YZ125-like virus has successively infected humans in Guangxi, Hunan, Zhejiang, and Jiangsu province from 2021 to date[5-7, 43], suggesting that these novel reassortants H5N6 viruses might get the ability to directly infect human without adaption.In view of the fact that the clinical manifestations of this novel H5N6 reassortant are acute encephalitis, rather than previous respiratory symptoms, once these reassortants obtained the ability of human-to-human transmission through reassortment or mutations, it will bring great health threat for human. Therefore, it is very urgent need to enhance the epidemiological surveillance of wild waterfowl and to take effective measures to prevent the close contact between wild waterfowl and poultry in areas where migratory birds frequently migrate.