#18,818
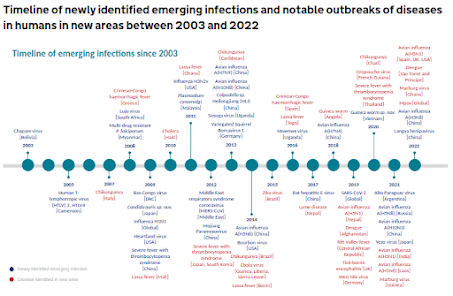
While avian flu continues to rank at - or near the top of - most people's pandemic threat lists, swine influenza viruses (which tend to spread stealthily in pigs) may actually pose bigger risks.
Unlike avian flu, these viruses are already well adapted to mammals, and in many ways porcine physiology is remarkably similar to that of humans (see The pig: a model for human infectious diseases).
Swine flu viruses are primarily H1, H2, and H3 subtypes; all of which have a long track record of sparking human pandemics (see Are Influenza Pandemic Viruses Members Of An Exclusive Club?).
Many of the viruses circulating in pigs today are decedents of human flu viruses which spilled over into swine over the years. This sharing of viruses is a two-way street.
Results. We estimate that the median multiplier for children was 200 (90% range, 115–369) and for adults was 255 (90% range, 152–479) and that 2055 (90% range, 1187–3800) illnesses from H3N2v virus infections may have occurred from August 2011 to April 2012, suggesting that the new virus was more widespread than previously thought.
H1N2 variant [A/California/62/2018] Jul 2019 5.8 5.7 ModerateH3N2 variant [A/Ohio/13/2017] Jul 2019 6.6 5.8 Moderate
H3N2 variant [A/Indiana/08/2011] Dec 2012 6.0 4.5 Moderate
Since 2010 we've seen more than 500 scattered reports of human infection with swine variant influenza viruses (H1N1v, H1N2v & H3N2v) in the United States, often associated with agricultural exhibits at county and state fairs.
But most of the world isn't bothering to test, or to share reports on, swine influenza.
While most swine influenza infections are due to H1, H2, or H3, there are outliers, including H5N1 (see Preprint: Bovine Derived Clade 2.3.4.4b HPAI H5N1 Virus Causes Mild Disease and Limited Transmission in Pigs).
Given their ability to concurrently carry multiple flu viruses, we've seen warnings (see Netherlands: Zoonoses Experts Council (DB-Z) Risk Assessment & Warning of Swine As `Mixing Vessels' For Avian Flu) that H5N1 could increase its pandemic threat by spreading (and evolving) in farmed swine.

Although we've only seen 1 swine-variant human infection reported so far in 2025 (see CDC FluView Week 5: Seasonal Flu Rising Again - 1 Novel (H1N2v) Flu Case In Iowa), summer and fall are prime time for spillovers.
Every summer the CDC reminds the public of the risks of swine variant flu infections (see twitter/X post) , which are often associated with state and county fair attendance.
First a link to their guidance page (follow the link for more resources), after which I'll have a brief postscript.
Take Action to Prevent the Spread of Flu Between Pigs and People Prevention
About
- Influenza A viruses circulate among many different animals. Influenza A viruses that circulate among pigs are called swine influenza A viruses.
- These viruses are different from influenza A viruses that spread among people and different from avian influenza A viruses.
- While rare, influenza A viruses--including seasonal human A viruses and swine influenza A viruses--can spread from pigs to people and from people to pigs. When an influenza A virus that normally infects pigs is found in people, it is called a 'variant influenza' virus infection.
- When people get variant flu, it's usually after contact with infected pigs or surfaces or environments contaminated with swine influenza A virus, such as a swine barn. These infections have occurred in different settings, including agricultural fairs.
- The Centers for Disease Control and Prevention (CDC) recommends people take the following actions to help prevent the spread of influenza A viruses between certain animals (including pigs) and people. While the content of this page focuses on pigs, similar precautions are recommended around poultry and dairy cows, which can carry and spread different influenza viruses called avian influenza A viruses.
Take Preventive Actions
- People at increased risk for severe influenza complications should avoid exposure to pigs.
- Don't eat, drink or put anything in your mouth in areas with pigs.
- Don't take toys, pacifiers, cups, baby bottles, strollers, or similar items into areas with pigs.
- Wash your hands with soap and running water before and after exposure to pigs outside or inside a swine barn. If soap and water are not available, use an alcohol-based hand rub.
- To further reduce the risk of infection, avoid or minimize contact with pigs in the pig barns and show arenas.
- Where possible, avoid direct contact with pigs that are known or suspected to be sick. If you must come in contact with pigs that may be ill, then wear personal protective equipment (PPE). This includes protective clothing, gloves, and a well-fitting mask that covers your mouth and nose. Parents and caregivers should review considerations for specific groups of people when selecting a respirator or mask for children.
- If you have a pig, watch for signs of illness (like loss of appetite, fever, tiredness, eye redness, discomfort, cough, or runny nose)If you suspect your pig is sick, call a veterinarian.
- If sick pigs are in an exhibition area, remove them right away.
- If possible, avoid close contact with sick pigs.
- Avoid contact with pigs if you have flu symptoms. Wait to have contact with pigs until 7 days after your illness started or until you have been without fever for 24 hours without the use of fever-reducing medications, whichever is longer. If you must have contact with pigs while you are sick, take the preventive actions listed above.
Like everyone else, people who care for pigs should get a seasonal flu vaccine every flu season. Although a seasonal flu vaccine probably will not protect people against infection with variant influenza A viruses (because swine influenza A viruses are substantially different from seasonal influenza A viruses that infect people), vaccination is important to reduce the risk of spreading human seasonal influenza A viruses to other people and to pigs. Seasonal flu vaccination might also decrease the potential for people or pigs to become infected with human influenza A viruses and influenza A viruses from pigs at the same time.
People at Higher Risk
- Anyone who is at higher risk of serious flu complications who plans to attend an event or setting where pigs will be present, such as an agricultural fair, should avoid pigs and swine barns.
- If people at higher risk cannot avoid exposure to pigs, they should wear a well-fitting mask that covers the nose and mouth (e.g., an N95 respirator or KN95 respirator if available, or if not available, a surgical mask) to reduce the risk of exposure to influenza viruses from pigs.
- People at higher risk of serious flu complications who develop flu symptoms should call a health care provider. Tell them about your risk factor and any exposure to pigs or swine barns you've had recently. Human seasonal flu vaccines will not protect against influenza A viruses that commonly spread in pigs, but prescription influenza antiviral drugs can treat infections with these viruses in people when treatment is started shortly after symptoms begin.
Recommendations for Fair Exhibitors
CDC guidance for people exhibiting animals including pigs, poultry, waterfowl, and cattle is available at Key Facts for People Exhibiting Pigs at Fairs.
While a swine variant pandemic might not prove to be as severe as one from an avian H5 or H7 virus, the likelihood of emergence of a swine-origin pandemic is considered higher.
This `longshot' status for H5N1 is illustrated in the following CDC IRAT chart, placing our current H5N1 virus in 11th place (emergence score) among their top 24 zoonotic influenza viruses with pandemic potential.
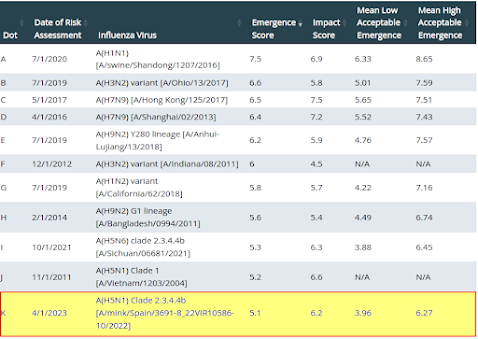
And of course, there are likely scores of other swine variants we don't know about, that are all own their own evolutionary paths. Most will be failures, but it only takes one over-achiever to change our inter-pandemic status quo.
Emerg Microbes Infect: A fatal Case of Acute Encephalitis Associated with a Novel influenza H3N2 Recombinant Virus Possessing Human-origin H7N9 Internal Genes
Eurosurveillance: Human Infections with Eurasian Avian-like Swine Influenza Virus Detected by Coincidence Via Routine Respiratory Surveillance Systems, the Netherlands, 2020 to 2023
Emerg. Microbes & Inf.: Eurasian 1C Swine Influenza A Virus Exhibits High Pandemic Risk Traits
Viruses: Isolation and Characterization of H1 Subtype Swine Influenza Viruses Recently Circulating in China