
#15,765
While it may seem an extreme response to those who live in countries where COVID-19 (and its variants) already run rife, nations - like Australia - that have managed to keep a lid on the pandemic for nearly a year are willing to take drastic actions to prevent its spread in the community.

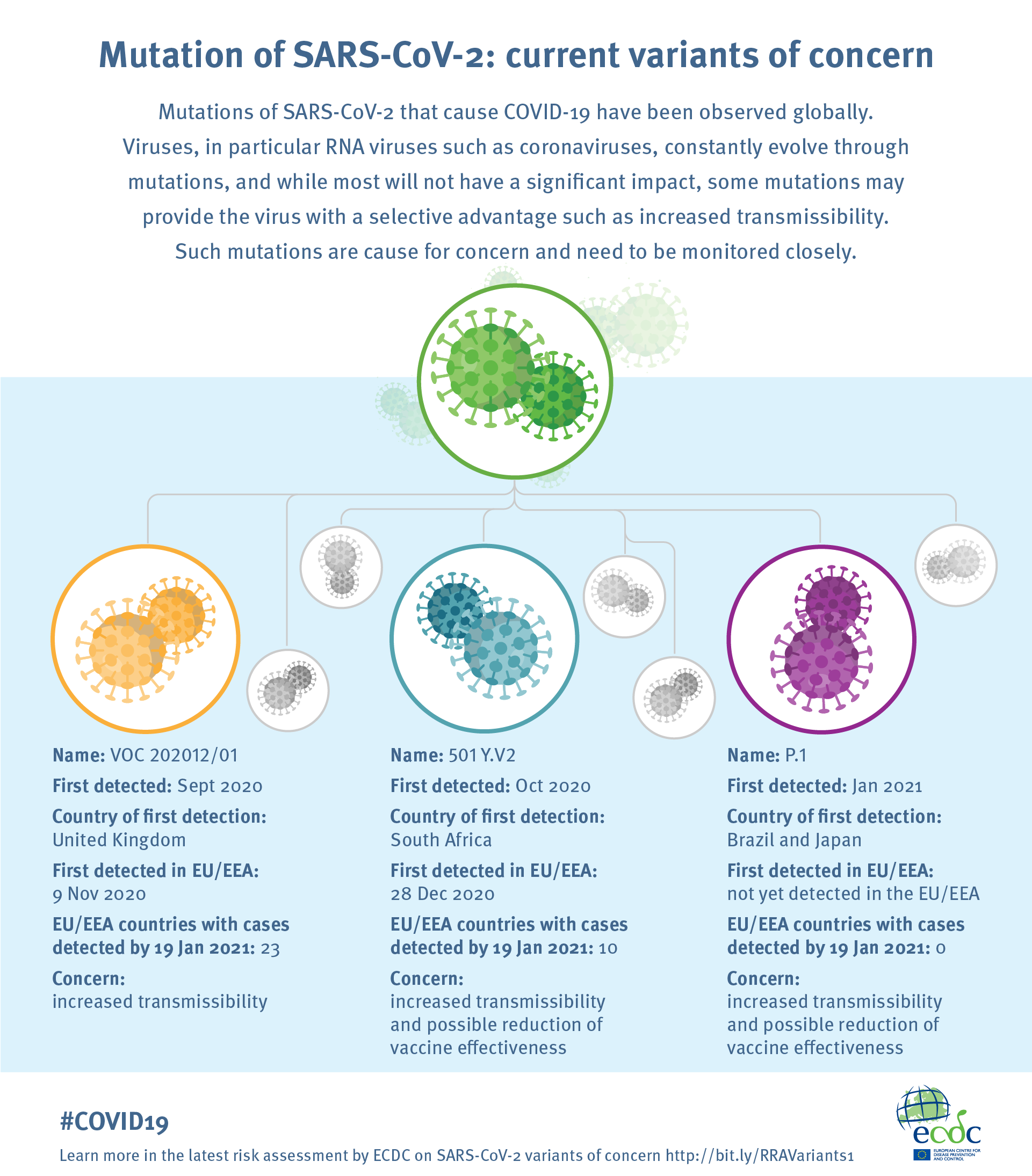
Two weeks ago we saw a huge response following the detection of the UK variant in a previously quarantined traveler in Brisbane (see Queensland: Incident Response Following Cluster Of COVID Variant B.1.1.7 In Brisbane Hotel), while today we are seeing a similar scenario unfold in Perth, nearly 3,600 km to the west.
This time, the lockdown is over a security guard who worked at a quarantine hotel - where at least one B.1.1.7 (UK) variant case is sequestered - who tested positive. While genomic sequencing hasn't been performed on the security guard's virus sample yet, authorities are taking no chances.
First the WA (Western Australia) Health Department announcement, followed by the WA government lockdown announcement.
COVID-19 update 31 January 2021
WA Health today confirmed that a security guard who works at a State Supervised Quarantine Facility (hotel) has been diagnosed with COVID-19.
The guard, a man in his 20’s, worked at the Four Points Sheraton Hotel on Tuesday 26 January, Wednesday 27 January, when he could have acquired the infection, and was diagnosed with COVID-19 overnight.
This indicates that the guard likely acquired the infection while at the hotel. Exactly how the infection was acquired remains under investigation.
He developed symptoms on Thursday 28 January and phoned in sick and did not go to work at the quarantine facility.
COVID-19 was detected following the man’s mandatory day seven swab.
He had tested negative for COVID-19 on January Friday 15, January Sunday 17 and Saturday January 23.
There is a known case of UK B.1.1.7 variant strain in quarantine at the hotel.
The man’s immediate household contacts have been contacted, tested and placed in isolation at State managed quarantine facilities to complete a 14-day quarantine period in a quarantine facility. All three have tested negative this morning.
The man was believed to be infectious at the following locations:
https://healthywa.wa.gov.au/Articles/A_E/Coronavirus/Locations-visited-by-confirmed-cases
Anyone who was at the above locations during the specified times is urged to attend a COVID-19 clinic for testing and remain in quarantine while awaiting the test result.
Close contacts will be contacted by public health officials and asked to quarantine for 14 days.
All State managed Covid clinics will increase staffing and extend their opening hours to cope with increased demand in the next few days.
This case will be reported in tomorrow’s case numbers, as the result came through following the end of the 24-hour reporting period.
The Department of Health reported no new cases of COVID-19 in yesterday’s reporting cycle. Today’s State’s total officially stands 902.
WA Health is monitoring 12 active cases and 881 people have recovered from the virus in WA.
Yesterday 519 people presented to WA COVID clinics – 514 were assessed and 514 swabbed.
To date 17 cases of variant strains have been detected (13 B.1.1.7 strain and 4 B.1.351 strain). Five of these cases remain active in hotel quarantine.
Visit WA Health’s HealthyWA website for the latest information on COVID-19.
Media contact: 9222 4333
Follow us on Twitter: @WAHealth
Note: The cases of variant strains reported above are not new cases. Genome sequencing – to define the strain of the virus – is a separate laboratory process carried out after someone who tests positive to COVID-19. All cases, regardless of strain, are managed by WA’s public health experts. The strains previously reported as the UK variant strain and South African variant strain will now be referred to as B.1.1.7 and B.1.351 respectively.
An updated breakdown of cumulative COVID-19 tests performed in WA will be released on Monday.
Details on the 5-day lockdown follow.
Perth, Peel and South West region enters lockdown from 6pm, 31 January 2021
Effective from 6pm tonight until 6pm Friday, 5 February 2021, the Perth metropolitan area, Peel and South West regions will enter a lockdown.
The following restrictions apply for the lockdown period:Masks are to be worn at all times when outside of your place of residence, this includes at workplaces and on public transport. For more information about masks, see the Healthy WA website (this is an external website).
- People should not leave Perth, Peel or the South West during this period
- People can enter Perth, Peel or the South West only to access or deliver essential health and emergency services and other essential requirements
- Non-residents currently in Perth, Peel and the South West are required to remain until the end of the restriction period however if you must leave for serious reasons you are to then return home immediately, stay home and get tested if symptoms develop
- Restaurants, cafes, pubs and bars to provide takeaway service only
- Elective surgery and procedures for categories 2 and 3 will be suspended from Tuesday, 2 February. Category 1 and urgent category 2 surgery will continue
- No visitors will be allowed in homes unless caring for a vulnerable person or in an emergency
- No visitors to hospitals or residential aged care and/or disability facilities
- No weddings permitted
- Funerals are limited to 10 people
- Travel remains prohibited within remote Aboriginal communities.
Schools will be closed for this week. Term 1, 2021 was due to start from February 1 but that will be postponed by one week.
The following facilities in the Perth, Peel and South West regions will need to close:
- Schools, universities, TAFEs and education facilities
- Pubs, bars and clubs
- Gyms and indoor sporting venues
- Playgrounds, skate parks and outdoor recreational facilities
- Cinemas, entertainment venues, and casinos
- Beauty therapy services, parlour or salon including hairdressers, barbershop, nail salon, tattoo parlour, spa or massage parlour
- Large religious gatherings and places of worship
- Libraries and cultural institutions
People will be required to stay at home unless they need to:The lockdown has been introduced due to the detection of a positive COVID-19 case in a hotel quarantine worker.
- work because they can’t work from home or remotely;
- shop for essentials like groceries, medicine and necessary supplies;
- medical or health care needs including compassionate requirements and looking after the vulnerable; and
- exercise within their neighbourhood, but only with one other person and only for one hour per day.
A list of locations the confirmed case visited is available on the Department of Health’s website (this is an external website). People who were at these places on these dates must go and get tested. Additionally, anyone who lives or works in the Falkirk Avenue Maylands shopping centre precinct should present for a test.
WA COVID clinic operating hours will be extended as part of a testing surge. Testing locations are available on the Healthy WA website (this is an external website).















{kind=link}