
#17,165
In 2005, the 194 member states of the World Health Organization (WHO) - following the reporting debacle surrounding SARS in 2002-2003 (see SARS and Remembrance) - approved the biggest change to the IHR (International Health Regulations) since 1969.
IHR 2005 required that all member nations develop mandated surveillance and testing systems and to report certain disease outbreaks and public health events to WHO in a timely manner (usually within 48 hours).
Although the agreement went into force in 2007, member states had until mid-2012 to meet core surveillance and response requirements. A great many nations - citing hardships - failed to meet that deadline, and a 2-year extension was granted.
In 2014, another extension was granted (see WHO: IHR & Global Health Security), and again in 2016.
The implementation of these standards is a big job, of course (see Ten things you need to do to implement the IHR), and requires a major commitment of money and resources by all member states. A job made difficult following the 2008 recession, and made worse by a war in Europe, growing international political tensions, and 3 years of a COVID pandemic.
Frustratingly, from Indonesia’s refusal to share H5N1 virus samples to the Saudi’s chronic foot dragging on MERS, to China's chronic belated reporting on avian flu, we’ve seen many examples where the spirit – and often the actual letter – of the 2005 IHR has been ignored by member nations.
Over the past 3 years the ongoing COVID pandemic seems to have become an excuse for many nations not to report on novel outbreaks. The WHO - which has limited enforcement options - often describes this diplomatically, as in their recent DON on MERS-CoV.
The number of MERS-CoV cases reported to WHO has substantially declined since the beginning of the ongoing COVID-19 pandemic. This is likely the result of epidemiological surveillance activities for COVID-19 being prioritized, resulting in reduced testing and detection of MERS-CoV cases.
The WHO, in almost every surveillance bulletin, reiterates the obligation of all nations to abide by the IHR (see below).
All human infections caused by a new subtype of influenza virus are notifiable under the International Health Regulations (IHR, 2005). State Parties to the IHR (2005) are required to immediately notify WHO of any laboratory-confirmed case of a recent human infection caused by an influenza A virus with the potential to cause a pandemic. Evidence of illness is not required for this report.
Yet we often only hear about novel flu cases months after-the-fact. And we have no way of knowing how many cases are never reported. For many countries - which would rather not deal with such things - don't test, don't tell is an attractive option.
With HPAI H5N1 spreading around the globe, with opportunities to reassort with other flu viruses, now is the time we need enhanced surveillance for suspicious flu infections (see UK APHA: Technical risk assessment for avian influenza (human health): influenza A H5N1 2.3.4.4b).
And while COVID has almost become a `routine' illness - with testing and reporting plummeting over the past 6 months - it is still capable of generating new, and potentially dangerous, variants (see WHO/FAO/OIE Joint Statement On Monitoring SARS-CoV-2 In Wildlife & Preventing Formation of Reservoirs).
While ignorance may be bliss, the next pandemic threat may be much closer than we think. We simply can't know what threats lie ahead if we don't proactively look for, and report, outbreaks.And what happens in China over the next six months could dramatically alter the trajectory of the pandemic, yet reporting from the Mainland remains as sparse and unreliable as ever.
But sadly - for a multitude of reasons - that doesn't happen nearly as often as it needs to. And if changes aren't made, we are likely to be caught unawares - and woefully unprepared - when the next pandemic threat emerges.
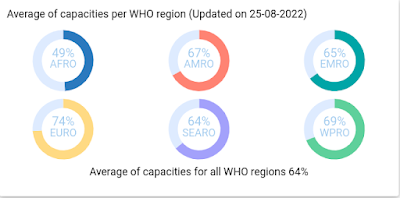
As the WHO IHR infographic at the top of this blog reminds us, `Until all sectors are on board with the IHR, no country is ready'.