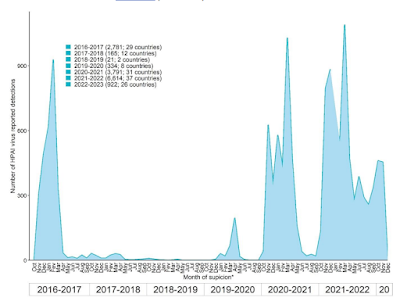
Waves of HPAI H5N1 clade 2.3.4.4b since 2016 - Credit ECDC
#17,290
Regardless of whether HPAI H5Nx can spark a human pandemic (still unknown), over the past 20 years we've seen roughly a thousand confirmed H5 infections around the world - predominantly in Asia and the Middle East - and undoubtedly many more have gone undiagnosed.
With zoonotic H5N1 (clade 2.3.4.4b) now widely dispersed around the globe, the virus has new opportunities to spill over into humans in countries that previously have seen little or no HPAI H5 activity.
Additional sporadic cases - even in the United States, Canada, or Europe - would not be unexpected.
As a result, countries like the United States, the UK, and other European nations have been releasing guidance for doctors, laboratory technicians, and public health officials on how to deal with potential cases.
Some of the recent risk assessments, and guidance documents, we've looked at include:
WHO Update & Risk Assessment On Human H5N1 Infection - EcuadorEarlier this month the British Columbia Medical Journal (BCMJ) released their own clinician's guide for dealing with suspected avian flu infections in humans.
WHO Rapid Risk Assessment on A(H5N1) clade 2.3.4.4b viruses (Includes 2 Severe/Fatal Human Infections)
UK HSA Technical Briefing: Risk Assessment On HPAI H5N1 & Human Infection
UK APHA: Technical risk assessment for avian influenza (human health): influenza A H5N1 2.3.4.4b
ECDC Guidance For Testing & Identification Of Zoonotic Influenza Infections In Humans In The EU/EAA
CDC On Preventive Measures to Protect Against Bird Flu Viruses
Avian influenza: A BC clinician’s guide to diagnosis and management
Issue: BCMJ, vol. 65, No. 1, January February 2023, Pages 27-28 BC Centre for Disease Control
By: Rohit Vijh, MD, MPH, CCFP Erin Fraser, DVM, MSc Mayank Singal, MD, MPH, CCFP, FRCPC
Highly pathogenic avian influenza (HPAI), notably of the H5N1 subtype, was detected in domestic poultry across BC and around the globe at unprecedented rates in 2022.[1-3] BC has had the highest number of poultry premises affected in comparison to other provinces,[1] leading to significant impacts on the livelihoods and well-being of poultry owners.Avian influenza viruses have sporadically infected humans and have largely followed direct exposure to infected poultry.[4] The rising detection among birds increases the potential for human exposure and intermixing of different influenza strains.[4] Human health risk is currently considered to be low. However, if the virus adapts and leads to sustained human-to-human transmission, this would be considered a high-impact event.[4] Early detection of avian influenza viruses in humans enables public health action to detect and control potential human-to-human transmission.Clinical presentation
Clinical signs and symptoms of avian influenza in humans closely resemble acute respiratory or influenza-like illness. Disease severity and manifestations can range from asymptomatic infection to severe.[5] Avian influenza viruses in circulation have an incubation period in humans of 2 to 10 days (with most averaging 2 to 5 days).[5]Who to test for avian influenza and report to public health
Clinicians should have a low threshold for testing patients presenting with symptoms compatible with avian influenza and who have had close contact with an infected/sick bird or animal or other concerning exposures[5] within 10 days following that exposure. These symptomatic individuals should be reported to your local Medical Health Officer as soon as possible.[5]How to collect specimens for avian influenza testing
When testing is indicated, a nasopharyngeal swab and a throat swab or sputum sample (for patients with a productive cough) should be collected.Notify the BCCDC medical microbiologist on call of the suspect case and testing request at 604 661-7033. Collect the sample and document the exposure on the test requisition (e.g., human high-risk HPAI), and send it directly to your local testing lab.Recommendations for management of HPAI exposure in humans
If asymptomatic
Provide instructions to self-monitor for the development of symptoms for 10 days after the last exposure, and report any symptom development immediately to local public health. Individuals should also be counseled to avoid visiting other farms, avoid interactions with individuals at higher risk of severe illness,[5] and avoid large gatherings for 10 days following exposure.
Individuals can be provided chemoprophylaxis for the purposes of protecting the individual and preventing further transmission. It can be given up to 7 days after the last exposure. Decision to offer prophylaxis should be based on clinical judgment and an exposure assessment. Exposure assessment should consider the use of personal protective equipment and whether any breaches occurred, the type of exposure (working directly with affected birds, working with birds with confirmed infection, open/closed air environment), the duration/time since exposure, and the risk of complications from influenza.[5]
If symptomatic
Antivirals should be considered for the treatment of both suspected and confirmed cases of avian influenza, as they can reduce the severity and duration of illness if administered within 48 hours of illness onset. The person should be advised to follow respiratory etiquette, wash hands regularly, and isolate from others for 7 days or until symptoms resolve, whichever is longer.
If household contacts develop symptoms before test results are available, they should also isolate and notify their local public health unit.
If the decision is made to provide chemoprophylaxis for contacts, oseltamivir 75 mg b.i.d. can be given for 7 days (for time-limited exposures) or 10 days (for ongoing exposures) in adults. Treatment of suspected or confirmed cases requires only a 5-day course. Alternate to oseltamivir could include zanamivir 10 mg b.i.d.[6]
What patients can do to protect themselves
Actions that people can take (particularly those handling birds and/or with small flocks) to protect themselves and others are provided in the interim BCCDC clinical guidelines.[5] To prevent co-infection with both seasonal human influenza and avian influenza viruses, it is important patients are offered the annual influenza vaccine.
—Rohit Vijh, MD, MPH, CCFP
Senior Public Health and Preventive Medicine Resident, UBCCommunity Family Physician
—Erin Fraser, DVM, MSc
Public Health Veterinarian, Public Health Response, BC Centre for Disease Control
—Mayank Singal, MD, MPH, CCFP, FRCPC
Physician Epidemiologist, Public Health Response, BC Centre for Disease Control
This article is the opinion of the BC Centre for Disease Control and has not been peer reviewed by the BCMJ Editorial Board.This work is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License
While future human infections with H5N1 are to be expected, unless and until the virus adapts well enough to transmit efficiently from human-to-human, its public health impact will be limited.
We've been seemingly on the brink several times with with H5N1, H5N6, and H7N9 viruses - and so far - none have manage to overcome that transmission barrier. Perhaps they never will.
But viruses have a superpower; the ability to evolve rapidly. What we can say about a virus today may not hold true tomorrow.
Which is why preparatory steps, like those listed above, are cheap insurance.